The choice to not take the COVID vaccine I feel is not defendable. The facts are that 99% of hospitalizations/deaths due to COVID are unvaccinated patients currently. This has caused a more severe strain on a already extremely stressed hospital staff, shortage of equipment and services, injury and death from other causes due to delay of care and suffering of everyone involved in the hospitalized COVID patient among other issues. Virologists report delta and other strains are accelerated and created due to the numbers of unvaccinated people in the US. The fact that vaccination rates have only increased about 20% since July with the information available is appalling, while there are 130k new infections daily in the US. This should not be a personal or individual choice and appears due to unfounded anxiety, medical or religious exception and or politics.
Specializes in Treatment-resistant Clinical Depression.
7 hours ago, MunoRN said:
We aren't already 'pushing' treatment of obestity and diabetes?
Are obesity and diabetes transmissible to others?
Not pushing hard like vaccines.
The obesity and diabetes aren't transmissible but teh avoidable costs are. The high cost of health care leads people to avoid doctor visits.
All this is a bit of a tangent, but every so often we hear about the costs of COVID care and the anti-vaxxer counterpoint is to introduce the tangent.
The transmissibility is the only reason to arguably justify forced medical procedures.
That said, raising health insurance rates for such risk groups might be worthwhile. I'm naturally immune. About to be forced into being vaccinated to secure the 4% advantage vaccines give and get 100% of teh risks, known and unknown. So...hurray for that.
Thing is, when there were rumblings about shared costs of care for COVID, my 4% chance of getting hospitalized would suddenly cost me money even though Vaccinated people had a 6% chance. I was not going to be reckless, but I would be treated as if I had no protection at all.
It wasn't scientifically valid reasoning, or fair. It was economic coercion. It was wrong. But it would've worked if President Pfizer hadn't put a gun to my career as an arm twist instead.
Obesity should come with higher premiums, but it'd be best to partner such sticks with the carrots of financial assistance so eating nutritious food less inclined to cause weight gain is affordable. Nutrition counseling to include food prep guidance could help. Therapy to counter self-medication of food as comfort could do a bit more.
Major tangent here, but it's important to share if we have a minute. Obesity can be treated, but it isn't free. Kind of like statistics classes in public school so people get a much better grasp of why vaccines are safer than actually catching the disease (unless you already caught it the first time, for which there is insufficient data concerning hospitalization and comorbidity contribution. Statistics giveth, and statistics taketh away.)
Specializes in Nurse Leader specializing in Labor & Delivery.
11 hours ago, capitalsfan83 said:
I get that. My whole point is that we are a country with certain freedoms. People should have a freedom to choose what they do with their body. You work in public health and probably deal with a lot of people that don't make good choices. Should we ban gay sex again? It endangers other people who don't have HIV / AIDS. Should we force them to take their antivirals and shun them if they don't? Should we ban alcohol so people don't drink and drive and put other people at risk? My family members were killed by a drunk driver. I can go on and on and on about this.
Are you ***ing kidding me with this? Um, 1985 called, and it wants its understanding of the AIDS epidemic back. Jesus ***ing christ.
Specializes in Nurse Leader specializing in Labor & Delivery.
9 hours ago, Seda8OR said:
Indefensible eh? Maybe when you have a friend die after the vaccine, and several others develop Central venous thrombosis and other issues a few days after being poked, you might reconsider your selfish demands
Maybe when you have a dozen friends who have died from Covid, and several others remain hospitalized for 3+ months, need lung transplants, and can't work due to long Covid and other issues after getting this deadly disease, you might reconsider your selfish demands.
Specializes in Treatment-resistant Clinical Depression.
21 minutes ago, klone said:
Maybe when you have a dozen friends who have died from Covid, and several others remain hospitalized for 3+ months, need lung transplants, and can't work due to long Covid and other issues after getting this deadly disease, you might reconsider your selfish demands.
See, this is counterproductive.
Outside of deep south states, this is statistically unlikely. The highest risk people (elderly, for example) have already vaxxed up and won't die.
700,000 people are going to die. .2% of teh population. 2 of 1000.
Dunbar's number suggests close ties to 150 people.
1 out of 6 people will lose someone they know well, but maybe not even all that well.
5 out of 6 will know someone who dies who was a casual acquaintance from their past perhaps. An ethereal, loose tie that just won't have a substantial impact.
When no one that an anti-vaxxer knows is dying, this kind of apocalyptical hysteria makes it sound like you don't know what you're talking about. I'm under the impression this is a big part of the problem. Anti-vaxxers trust only what their eyes can see and don't appear to incorporate statistics. Proper risk assessment of loved ones dying might help to recognize the avoidable, potentially enormous cost of not taking an easy precaution against your own misery lottery ticket coming in.
Vaccination rates have climbed in low vax areas, I strongly suspect, only because deaths have increased to the point where the circle is closing in on them and their eyes can see that the warnings weren't just vax shilling. I wish so much glaring, costly proof hadn't been necessary.
Specializes in Psych, Addictions, SOL (Student of Life).
5 hours ago, imppress said:
Not pushing hard like vaccines.
The obesity and diabetes aren't transmissible but teh avoidable costs are. The high cost of health care leads people to avoid doctor visits.
All this is a bit of a tangent, but every so often we hear about the costs of COVID care and the anti-vaxxer counterpoint is to introduce the tangent.
The transmissibility is the only reason to arguably justify forced medical procedures.
That said, raising health insurance rates for such risk groups might be worthwhile. I'm naturally immune. About to be forced into being vaccinated to secure the 4% advantage vaccines give and get 100% of teh risks, known and unknown. So...hurray for that.
Thing is, when there were rumblings about shared costs of care for COVID, my 4% chance of getting hospitalized would suddenly cost me money even though Vaccinated people had a 6% chance. I was not going to be reckless, but I would be treated as if I had no protection at all.
It wasn't scientifically valid reasoning, or fair. It was economic coercion. It was wrong. But it would've worked if President Pfizer hadn't put a gun to my career as an arm twist instead.
Obesity should come with higher premiums, but it'd be best to partner such sticks with the carrots of financial assistance so eating nutritious food less inclined to cause weight gain is affordable. Nutrition counseling to include food prep guidance could help. Therapy to counter self-medication of food as comfort could do a bit more.
Major tangent here, but it's important to share if we have a minute. Obesity can be treated, but it isn't free. Kind of like statistics classes in public school so people get a much better grasp of why vaccines are safer than actually catching the disease (unless you already caught it the first time, for which there is insufficient data concerning hospitalization and comorbidity contribution. Statistics giveth, and statistics taketh away.)
I haven't read all the posts so I apologize if you already answered this question. How was it determined that you are naturally immune?
Guillain-Barré syndrome (GBS) is a side effect of the vaccination. Hopefully you don't have that and your symptoms subside. Call on God, but row away from the rocks.
I was thinking of Cuada equina because the left side of my private area was numb also, but yesterday during a nap it spread over my chest. I pray it goes away
Our whole system is based on “sick care”. You’re fat? OK we have a pill for that! There is an interest but whatever is being done is obliviously not working. We keep getting bigger and fatter as a nation.
No kidding. This is news to no one and almost everyone can write a.book on the reasons and why we can't get handle on them. But what does this have to do with the topic? it would be a good thread to start if you like but most of us already understand that our payment system is skewed to procedures, not patient teaching (which the doctors shouldn't be doing anyway. That role should be filled by RN'S.
The only way anyone should. A positive COVID test, especially after being dog sick for a few days.
Being sick at about the right time and assuming it was COVID? Yeah, daft madness.
You've referenced a couple of times that you are naturally immune, which without qualifying that as being a transient immunity, seems like something others could interpret as meaning they will never need a vaccine, which is a bit dangerous. Neither previous infection or vaccination provides long lasting immunity.
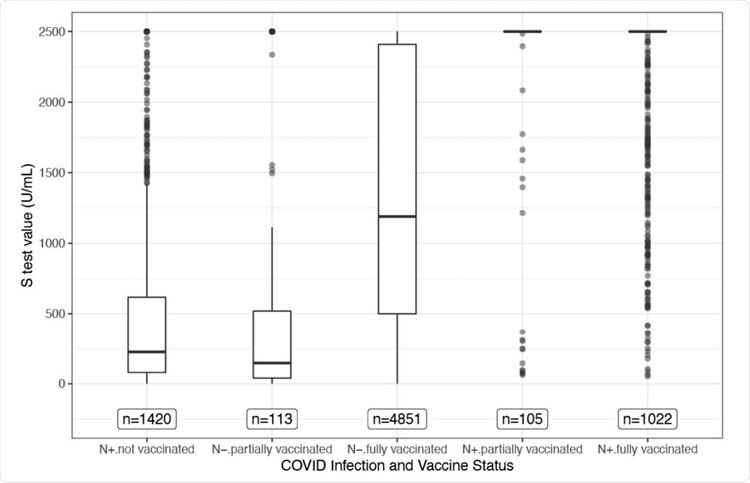
Texas has a large project tracking how antibody levels compare based on previous infection and vaccination status. The bar graph on the far left represents those with previous infection and unvaccinated. The bar represents the 25th to 75th percentile of people, likely the first wave of infections last nov-jan, with the outliers distinctly separated, likely representing early infections in the current wave. Those in the wave of about 9 months ago have antibody levels that are near or below the level considered sufficient to be reasonably protected.
Specializes in Treatment-resistant Clinical Depression.
22 minutes ago, MunoRN said:
You've referenced a couple of times that you are naturally immune, which without qualifying that as being a transient immunity, seems like something others could interpret as meaning they will never need a vaccine, which is a bit dangerous. Neither previous infection or vaccination provides long lasting immunity.
Texas has a large project tracking how antibody levels compare based on previous infection and vaccination status. The bar graph on the far left represents those with previous infection and unvaccinated. The bar represents the 25th to 75th percentile of people, likely the first wave of infections last nov-jan, with the outliers distinctly separated, likely representing early infections in the current wave. Those in the wave of about 9 months ago have antibody levels that are near or below the level considered sufficient to be reasonably protected.
After Provincetown, the expecytation of vaccine preventin g sickness were no longer a ready boast.
Suddenly hospitalization is all that mattered and it was still great to get vaccinated because you'd avoid the hospital, even if you did get sick.
I was actually okay with that. We don't mandate the flu shot because it "only" kills 60,000 per year. Most in high risk groups.
We don't care much about flu infections, as annoying as they are.
The previous wisdom claimed the vaccine was stro9nger protection because of higher antibodies than naturally immune people.
Come to find out that naturally immune people are seriously sick with COVID (getting reinfected, in the case of the naturally immune) 2% less often, despite lower antibodies.
So if naturally immune people have lower antibodies now, I dare say I care even less about low antibodies than I do about infections, which I care less about than hospitalization.
The low antibody counts troubled me in March, until we got more relevant data to determine the correlation of high antibodies and low hospital admission is sketchy, to be charitable.
It would seem other factors (T and B cell activity?) are critically important to avoiding hospitalization because natural immunity has been proven to be stronger and longer lasting. Provincetown victims had less than six months between vaccination and serious (but not hospitalization-worthy) illness. If naturally immune patients' immunity petered out so quickly, you don't think we would have heard about that from the CDC and the vaccine manufacturers?
The Israel data seems to indicate naturally immune people are in pretty good shape (subject to the same comorbidities that kneecap vaccine efficacy)
We aren't already 'pushing' treatment of obestity and diabetes?
Are obesity and diabetes transmissible to others?
Does obesity and diabetes need to travel in droplets before we care about how many people die from it and the other associated complications?
Just because it isn't spread by droplet doesn't mean it isn't contagious.
None of the points anyone is making is designed to dismiss the dangers of COVID rather to question why we are selective with mandates based on the notion the mandate is intended to save lives.
Specializes in NICU, PICU, Transport, L&D, Hospice.
25 minutes ago, jive turkey said:
None of the points anyone ismaking is designed to dismiss the dangers of COVID rather to question why we are selective with mandates based on the notion the mandate is intended to save lives.
This thread is about remaining unvaccinated and how indefensible that choice is for the vast majority of the unvaccinated. Your inability to comprehend why public health priorities focus on a contagion currently in pandemic status is well documented but off topic.

imppress
15 Posts
Not pushing hard like vaccines.
The obesity and diabetes aren't transmissible but teh avoidable costs are. The high cost of health care leads people to avoid doctor visits.
All this is a bit of a tangent, but every so often we hear about the costs of COVID care and the anti-vaxxer counterpoint is to introduce the tangent.
The transmissibility is the only reason to arguably justify forced medical procedures.
That said, raising health insurance rates for such risk groups might be worthwhile. I'm naturally immune. About to be forced into being vaccinated to secure the 4% advantage vaccines give and get 100% of teh risks, known and unknown. So...hurray for that.
Thing is, when there were rumblings about shared costs of care for COVID, my 4% chance of getting hospitalized would suddenly cost me money even though Vaccinated people had a 6% chance. I was not going to be reckless, but I would be treated as if I had no protection at all.
It wasn't scientifically valid reasoning, or fair. It was economic coercion. It was wrong. But it would've worked if President Pfizer hadn't put a gun to my career as an arm twist instead.
Obesity should come with higher premiums, but it'd be best to partner such sticks with the carrots of financial assistance so eating nutritious food less inclined to cause weight gain is affordable. Nutrition counseling to include food prep guidance could help. Therapy to counter self-medication of food as comfort could do a bit more.
Major tangent here, but it's important to share if we have a minute. Obesity can be treated, but it isn't free. Kind of like statistics classes in public school so people get a much better grasp of why vaccines are safer than actually catching the disease (unless you already caught it the first time, for which there is insufficient data concerning hospitalization and comorbidity contribution. Statistics giveth, and statistics taketh away.)