I'm a senior nursing student and this debate arose with a couple of my classmates and me. I work as an ER tech and they work as patient care techs on the floor. As of right now, CDC guidelines state for PPE:
Quote
Updated PPE recommendations for the care of patients with known or suspected COVID-19:
Based on local and regional situational analysis of PPE supplies, facemasks are an acceptable alternative when the supply chain of respirators cannot meet the demand. During this time, available respirators should be prioritized for procedures that are likely to generate respiratory aerosols, which would pose the highest exposure risk to HCP.
Facemasks protect the wearer from splashes and sprays.
Respirators, which filter inspired air, offer respiratory protection.
When the supply chain is restored, facilities with a respiratory protection program should return to use of respirators for patients with known or suspected COVID-19. Facilities that do not currently have a respiratory protection program, but care for patients infected with pathogens for which a respirator is recommended, should implement a respiratory protection program.
Eye protection, gown, and gloves continue to be recommended
So basically CDC is saying wear an N95 if you have it, but if you don't, wear a surgical mask until you can get an N95.
So if you have a suspected or confirmed COVID-19 patient, and all you have is a surgical mask and no N95, can you refuse to take care of that patient? Do you face any legal repercussions or potential fallout from your employer if you do refuse? Asking not only about tech positions, but RN positions as well.
I would understand that concern more if it were coming from the recommendation of the hospital - I wouldn't trust them and would likely assume they were just being cheap. But overall I believe the CDC to be a reliable source and don't believe they would put out a recommendation like that if it were not sound advice.
Cheap and not wanting to see staff walk out en masse, thus forcing managers to work the bedside.
To clarify, the CDC has not said that procedure / surgical masks are just as safe as an N95 or other respirator, they specifically state this is not true. They have also not said that there are certain circumstances when caring for a COVID patient where a procedure or surgical mask provides reliable protection.
What they've said is that when the appropriate level of respiratory protection is not available, then procedure / surgical masks are better than nothing at all, and actually now they're saying when those run out then use a scarf or bandana. That doesn't mean they're saying a scarf or bandana is as effective at stopping 5 micron droplet nuclei as well as an N95 mask.
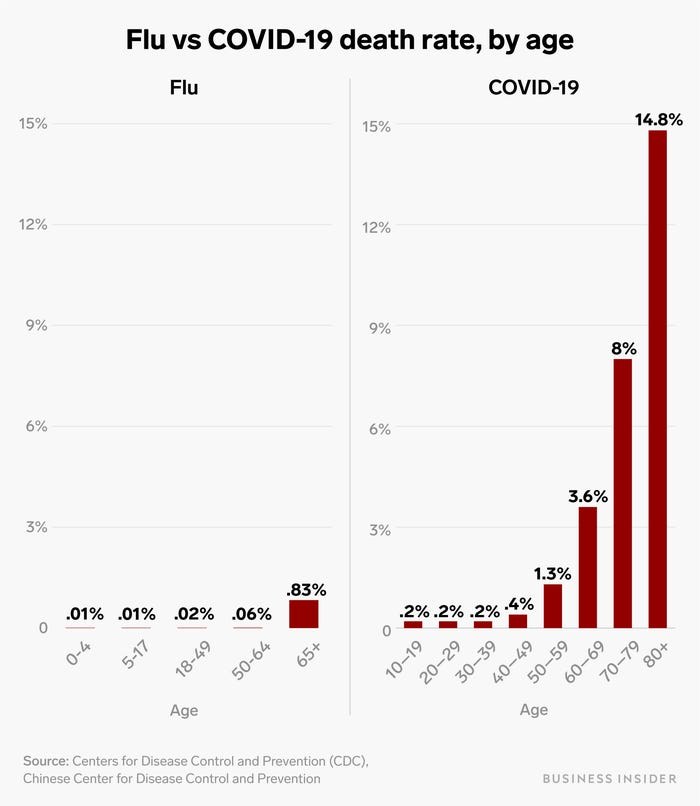
Younger people are certainly not immune from COVID-19, but there is a clear increase in mortality risk with an increase in age with this virus.
I’m just saying that at my hospital we have different levels of risk, therefore different levels of PPE. With there being a shortage, they have evaluated the greatest threat to healthcare workers and those are the ones that will wear the N95 masks. A PUI is treated differently than a confirmed, intubated case.
Use your professional assessment/reflection model here...
it makes zero sense to do that, since you could spread the virus to others.
No protection, No care.
I see no way that legally they could take away licenses for that. They are using pressure to make nurses face this in unsafe ways because they are afraid of the breakdown of the hospital/healthcare system.
Use LOGIC, there have already been amazing doctors and nurses that have died. So sad. I'm following the CDC recommendations and ensuring my family who has a member that is on an immunosuppressant is not exposed. I choose to do this to protect her. It is a moral option, not a moral obligation.
I'm trying to Google it now and can't find anything. But when I wasn't looking for this particular statistic this week, I came across 2: one was 8% and one was 10% of health care professionals who got Covid in Italy. Of course, we can never know whether they picked it up at work or not. I don't know anything about the rate of differences between Covid testing in the community vs. the hospital. But it was a reason contributing to the systemic hospital overload and possibly to the death rates. Imagine if 10% of our staffing here just disappeared from work.
Earlier today I saw video of an Italian ER overflowing with Covid patients, to include people lining the hallways. One thing that impressed me was how crowded the entire filmed area was and all the healthcare workers at work going from patient to patient. They looked very, very stressed. Not surprising that in these conditions, many would themselves become infected.
Let's be honest. Newest data in strict testing labs have shown this thing hangs around in the air for up to three hours (burst-test--simulating aeorsolized particles from procedures and or strong coughs and sneezes). Similar to SARS 1, actually.
Let's also be honest that hot spots like Italy and Wuhan have their frontline workers in full head-to-toe hazmat garb.
Let's also be honest that the corporate model of healthcare in the US combined with decades of outsourcing the means of production have left our hospitals woefully understocked for PPE.
It is what it is and we'll have to do the best we can to protect ourselves, our families, and our patients. I mean, we signed up to take care of people.
That said, I know of no firefighter that signed up to rush into burning buildings in their underwear and a pair of goggles.
Neither did we sign up to walk into viral plumes unprotected..
Health care workers are dying from this. Young, and not-so-young alike.
We in the US are going to have to get veeeery creative until mass production of PPE begins.
Let's be honest. Newest data in strict testing labs have shown this thing hangs around in the air for up to three hours (burst-test--simulating aeorsolized particles from procedures and or strong coughs and sneezes). Similar to SARS 1, actually.
That test artificially kept the particles in the air to see whether they could remain viable while artificially kept in the air. The answer was yes. But when allowed to drop to the ground, they did leave the air. The virus stays viable on inanimate objects; we know that.
Healthcare workers are physiologically comparable to non-healthcare workers when it comes to how our bodies are affected by a virus. It's not as though our mortality risk is not comparable because of our third lung.


NormaSaline
1 Article; 142 Posts
Maybe someone can post statistics about COVID-19 infection rates, complications, hospitalizations among HCW.