I'm a senior nursing student and this debate arose with a couple of my classmates and me. I work as an ER tech and they work as patient care techs on the floor. As of right now, CDC guidelines state for PPE:
Quote
Updated PPE recommendations for the care of patients with known or suspected COVID-19:
Based on local and regional situational analysis of PPE supplies, facemasks are an acceptable alternative when the supply chain of respirators cannot meet the demand. During this time, available respirators should be prioritized for procedures that are likely to generate respiratory aerosols, which would pose the highest exposure risk to HCP.
Facemasks protect the wearer from splashes and sprays.
Respirators, which filter inspired air, offer respiratory protection.
When the supply chain is restored, facilities with a respiratory protection program should return to use of respirators for patients with known or suspected COVID-19. Facilities that do not currently have a respiratory protection program, but care for patients infected with pathogens for which a respirator is recommended, should implement a respiratory protection program.
Eye protection, gown, and gloves continue to be recommended
So basically CDC is saying wear an N95 if you have it, but if you don't, wear a surgical mask until you can get an N95.
So if you have a suspected or confirmed COVID-19 patient, and all you have is a surgical mask and no N95, can you refuse to take care of that patient? Do you face any legal repercussions or potential fallout from your employer if you do refuse? Asking not only about tech positions, but RN positions as well.
My state has addressed the issue of whether nurses can refuse to care for these patients, the response was that you're free to permanently surrender your license, but that's the only option.
I would argue that older and immunocompromised nurses should be more of a last choice for caring for COVID patients, although we might already be to that point.
Pretty much every “state” worker in my state is sitting inside an office that’s not open to the public, not being coughed on by presumptive positive patients.
despite the double-speak, every situation will have additional circumstances that aren’t addressed neatly in one handy package..
my clinic (dialysis) has been designated by management to run an extra shift at to take all positive and presumptive positive patients from the area, possibly seeing the first positive patient in the coming week.
the n95’s are still safely locked up, and we’re triaging in the lobby with surgical masks (2 per day).
I’m personally a bit fatalistic in thinking that staff including myself were probably infected months ago- we had a wave of nasty respiratory illness amongst the staff that most worked with due to already short staffing.
The issue of morality and obligation is quite complex - whilst I did willingly engage in an occupation that would occasionally expect to treat patients that are infected with various things, the *setting* I chose was ambulatory and distinctly “non acute”, so I’ve repeatedly been told when applying for other positions.
The definition of “ambulatory” and “non-acute” has repeatedly been stretched to levels that were quite comical during good times, and staffing levels were already 50% higher than any state that cares to regulate staffing has chosen for themselves.
Our local hospitals have been dumping patients who were too sick to be released on us and on “lower level” care facilities for my entire career here as a matter of practice and routine. Interestingly, my clinic has been getting “dinged” by Medicaid for “re hospitalizations” as a matter of routine as well - this fact is exceedingly well documented on a board in our break room.
Amazingly, no one has connected the dots to realize that the reason why patients are getting “re-hospitalized” at alarming rates is because they were too sick to be discharged in the first place.
I’m personally grappling with the decision of whether to accept the “new deal” of *importing* positive patients from other clinics to my clinic over the next few days, and I’m understandably bristling at the implications that there’s some sort of “obligation” to surrender my income and livelihood if I make the perfectly rational and reasonable decision to not *knowingly* expose myself and my own family to something that may well kill them - myself and my family are both older and respiratory compromised.
if my employer hadn’t already “poisoned the well” by intentionally understaffing, underpaying, and by locking up the masks that might actually protect me from illness, my obligations to them might be more clear. If my state authorities had not been bought off by my employer’s big-money lobbying against safe staffing in good times, I might trust them more now.
At this point, the dilemma is simply one of my genuine need to serve my patients and to get them through this balanced against the need to keep myself in the game as the days get darker - and I honestly haven’t made a decision where the line is drawn yet.
If the state (or my peers) wish to judge me for whatever final decision is made, I’ll demand an in-person trial & I believe that the jury needs to be wearing the same paper masks I’m triaging in, I get to shake your ungloved hands before you retire to deliberate, and I’ll warn you that I have a persistent cough.
if my employer hadn’t already “poisoned the well” by intentionally understaffing, underpaying, and by locking up the masks that might actually protect me from illness, my obligations to them might be more clear. If my state authorities had not been bought off by my employer’s big-money lobbying against safe staffing in good times, I might trust them more now.
I couldn't agree more. Being treated as a necessary but inconvenient cost burden hardly inspires selflessness and sacrifice. That makes, in my eyes, those who choose to stay and take the informed risk all the more heroic (casting no shade on those who for whatever reason choose not to stay). Times were strange already with corporations wanting to be granted the same rights as people while their employees are treated like disposable pawns in a profit and loss game. Utterly bizarre that those same corporations now expect the pawns to morph into martyrs.
Has anyone else here read this: https://www.deaconess.com/How-to-make-a-Face-Mask? We are certainly doomed when a Harvard affiliated hospital is releasing this kind of cranckery. I associate cloth masks with hand-cranked ice cream makers made out of wood. Boy, that ice cream tasted great! Is the CDC being told what to release by the White House to distract us from the fact that we were so unprepared for something just around the corner for years?
Has anyone else here read this: https://www.deaconess.com/How-to-make-a-Face-Mask? We are certainly doomed when a Harvard affiliated hospital is releasing this kind of cranckery. I associate cloth masks with hand-cranked ice cream makers made out of wood. Boy, that ice cream tasted great! Is the CDC being told what to release by the White House to distract us from the fact that we were so unprepared for something just around the corner for years?
The CDC is saying - responsibly, I think - that in the absence of an approved mask a scarf, a bandana or (by inference) a home made mask is better than nothing. The Deaconess post makes it seems there are CDC approved designs. Not so.
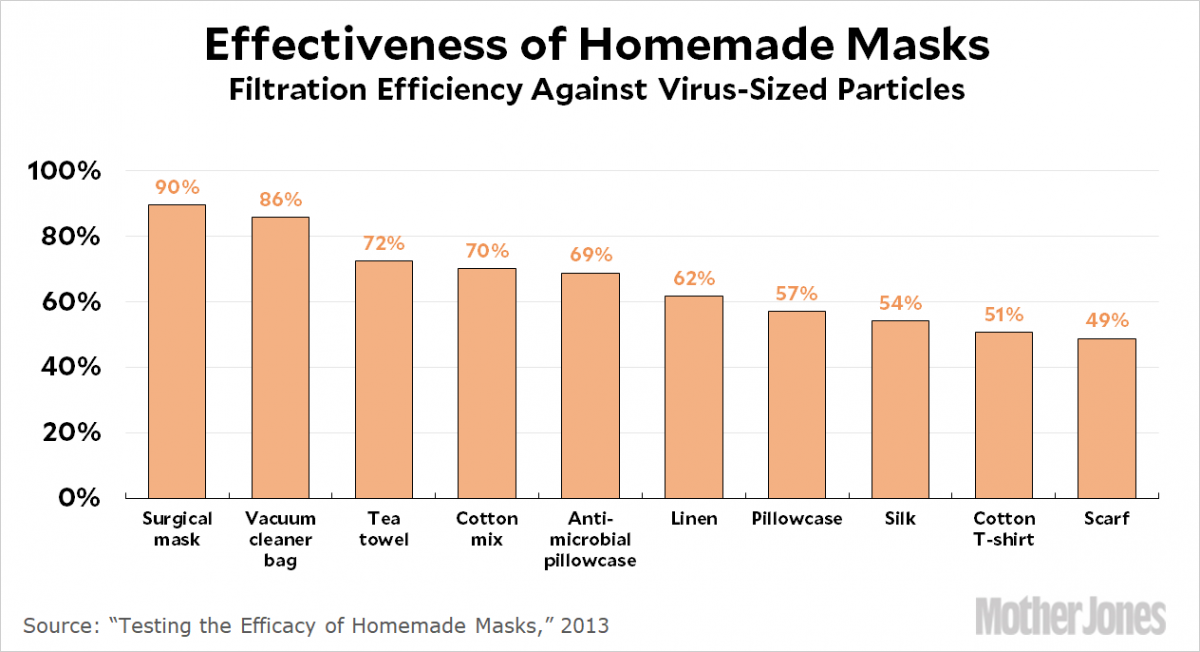
There's a chart out there showing the % of viral particles various materials filter. HEPA fabric is way up there, but unfortunately you can't breathe through it. The cloth people are making masks out of in there homes filters around the 50% range. In fact non-N95 masks in general are far better for keeping the wearer from spewing droplets into the air than they are for protecting a wearer.
I've made a bunch of masks but am only giving them to people I can specifically tell that they won't protect you from COVID-19.
Yep, admin will certainly throw you under the bus. Ask them to volunteer to help during the surge without adequate PPE. See how many volunteers you get. Also don't forget that the vast majority of the executives are better paid than you for a job with very little personal risk.
Any RN's that actually accept that it is OK to work without proper protective equipment are not thinking wisely. Healthcare workers have died from the virus. Don't be one of them and if you do not get the right high level PAPRs, you have every right to protect yourself and walk out. Do it for your kids, family, and for all nurses...because it is not smart as profession to accept unsafe work environments ever...If you do you should be getting paid a lot more an hour, in my opinion.
Maybe they need to create a new job description - Pandemic RN willing to work without the proper safety equipment with high risk of contracting virus, 200 dollars an hour sounds about right - even then, I would not show up for my shift or sign up for that job. No way.
Just wondering, what does a nurse anesthetist make per hour sitting in an OR. Not to say that they shouldn't be well compensated but shouldn't those risking there lives and their families be well compensated also?
Specializes in Critical care, tele, Medical-Surgical.
In my state a registered nurse may refuse to care for one or more patients without losing his or her license. That nurse may, and often will be terminated.
Quote
Generally for patient abandonment to occur, the nurse must:
a) Have first accepted the patient assignment, thus establishing a nurse-patient relationship, and then
b) Severed that nurse-patient relationship without giving reasonable notice to the appropriate person (e.g., supervisor, patient) so that arrangements can be made for continuation of nursing care by others.
A nurse-patient relationship generally begins when responsibility for nursing care of a patient is accepted by the nurse....
My state has addressed the issue of whether nurses can refuse to care for these patients, the response was that you're free to permanently surrender your license, but that's the only option.
I would argue that older and immunocompromised nurses should be more of a last choice for caring for COVID patients, although we might already be to that point.
This decision was made, of course, by people who will never have to go anywhere near the bedside. Typical bullying of our profession.
Pregnant and breastfeeding women should also be exempt, although I guess they could volunteer if they wish to do so.


Gampopa
180 Posts
Here's another link to a good research backed article on spread of COVID19 and use of PPE:
http://www.cidrap.umn.edu/news-perspective/2020/03/commentary-covid-19-transmission-messages-should-hinge-science