well,actually in our center pain scale score just been practiced and i'm still a young baby in getting pain scale score..and i even do not know / not confident in asking patient that in pain for their pain score.sometimes i get scolded because of asking for 'how much pain does he/she suffered'...
can you'll guys give me some 'nice' way of getting pain scale score?because i know you'll expert in this..
"Are you in any pain?" (if they already said they are in pain, I will skip this)
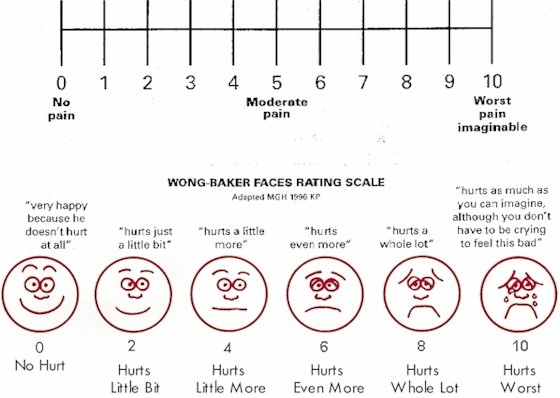
If yes, "on a scale of zero to ten, with zero being no pain, ten being the worst pain imaginable, how would you rate that pain?" It seems like the 20 year old with a sore throat will be a 10, an 80 year old with a broken hip will be about a 2...only when they move it. Either way, chart what they say. Our EHR has a point and click pain scale 0..1..2...etc...10...>10. Many people (often the really bad sore throats) will rate it at "10,000" or something similar. I will chart >10.
If they are in pain "how would you describe that pain?" If they ask for what I mean, I will say "an ache, burning, sharp, cramping..." I don't like to say that right off because I don't want to influence their description. Usually, though, they get what I mean and offer a descriptor.
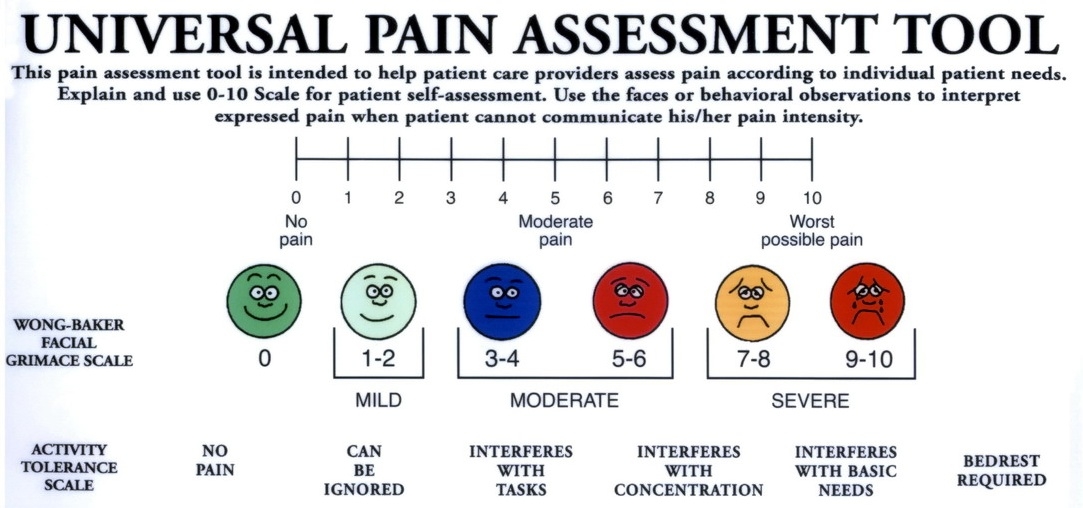
I ask to rate on a scale of 0 - 10 with 0 being no pain and 10 being that is the only thing they can concentrate on. It's the best I can think of but I still get patients laughing on their cell stating their pain is a 10
I think a mistake is comparing all pain as the same no matter the cause or use the same pain scale for any and all pain. "Zero is no pain....10 is someone sticking a burning stick in your eye."
I tolerate a lot of pain. Yet I will never forget about 6 years ago I had a sore throat. Well......it is "just a sore throat" so I can't think I would tell anybody it is "being burnt alive or the worst pain I can imagine" yet on a scale of 1 - 10 just comparing sore throat pain to no sore throat pain I would say it is a 10.
I wish I could explain it better.....does that make any sense to anyone?
You can't compare all pain the same.
Anyway most of the time I just ask the patient if it hurts a little or a lot and make up my own numbers because I hate the pain scale.
Specializes in PICU, NICU, L&D, Public Health, Hospice.
Yeah I know. Thats why im saying to me a 10 is that. Sheesh.
And of course, my comment was reflecting the fact that you were identifying what a pain of 10/10 is to YOU, with a "sigh" relative to their (the patient's) interpretation.
The reality is that when it comes to the patient's pain and qualification of such there is NO relationship to your personal experience with pain. Our personal qualification of pain levels is of NO relevance to the patient's description or qualification of their pain.
So comments that suggest that the patient may exaggerating their pain level based upon our opinion of what their response should be (as compared to our own) is an unprofessional assessment of pain which puts our subjective thoughts on pain before the patient's. IMHO
PS I have clarified my thoughts. Compare their pain to their pain. I say "If when your abdominal cramps were their worst it was number 10, what number is it now." Or "when your chest pain was it's worst it was a 10 what number is it now." Or "If when your cramps (for woman) were their worst was number 10 what number is it now." Etc.
The pain scale is a joke! You are either in pain or your not! Patients look at you like you are crazy how can you put a number on it, its either a little or a lot! Get real!
I used to ask what it was 0-10, zero being none and ten being hit by a truck. One day my patient responded "Well, it's not nearly as bad as the time I was hit by a truck...."
- I do not usually medicate, unless patient requests (some patients are medicated round the clock at home to keep pain levels low, so used to it and will request meds while in hospital, watching clock, so medicate them as long as within parameters and VS/cognition/arousability within normal limits.
- may reposition &/or apply cold or heat, etc. for comfort
3-4: mild discomfort/pain
- Medicate if patient requests it. If not, advise patient to call if he/she feels pain is getting worse.
5-6: I feel it, I am very uncomfortable. I need something to take the edge off this pain.
- Definitely want to stay on top of it. If patient refuses pain meds, educate as to pain, pain control, need for pain relief, etc, and continue to monitor.
7-8: I am in severe pain.
- Definitely needs pain meds.
9-10: I am in "excruciating, mind-numbing, I am about to go into shock from the pain" pain
- definitely medicate
- monitor closely...VS? Cognition? Arousability?
For patients who consistently smile, laugh, joke, on phone, eating, walking all over the unit while maintaining 10/10 pain level, I use both the 0-10 and the FLACC score.
If pain remains high &/or unrelieved, I discuss calling for new orders/changing meds w/doctor. I have had a few patients who, when informed that if pain med is not working it is my duty to call and get new orders/new meds/whatever, will suddenly state that their pain has finally eased a little from that narcotic that had not touched their pain all shift long



7feetunder
54 Posts
yeap,agreed.
this guy answered me with smiling face "my pain?10."
~hmmm..~