The legislators may raise the question of another nurse staffing bill nurses are lobbying.
It is very confusing for legislators to navigate WHY these bills are different. You can assist them!
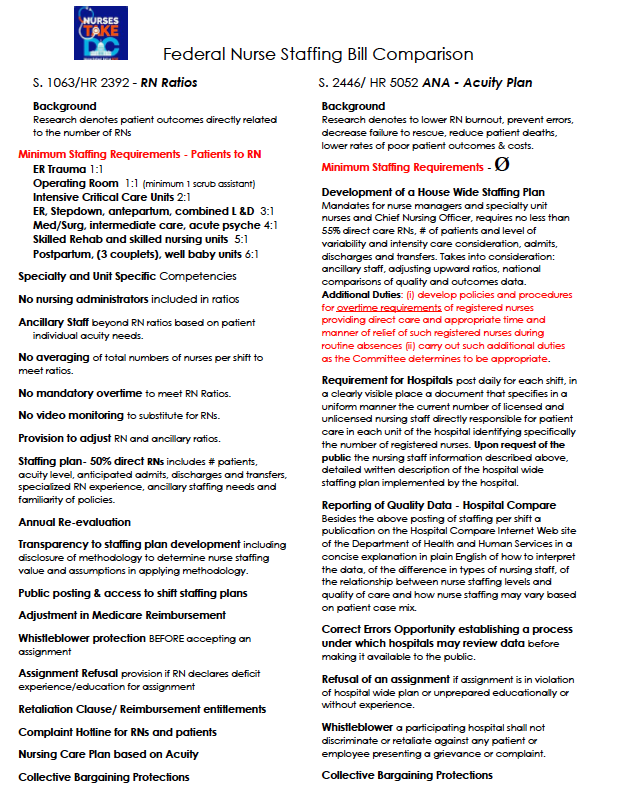
Our RN Ratio bills S. 1063/HR 2392 has the mandatory minimum nurse staffing ratios. The American Nurses Association bills S. 2446/HR 5052 share the importance that patient outcomes are directly affected by numbers of RN staff, but that is where the similarities seem to end.
Bottom line difference is in the ANA bill, no regulatory mandate that the employer to commit to a staffing plan in writing to begin any shift. Look at the Side by Side and you can always read each bill fully to get the flavor of the missing employer commitment to staff even though they agree fully with the research as we do: adequate numbers of nurses and support staff provides the patient with better outcomes.
Visit nursestakedc for information on the movement #NursesTakeC