The legislators may raise the question of another nurse staffing bill nurses are lobbying.
It is very confusing for legislators to navigate WHY these bills are different. You can assist them!
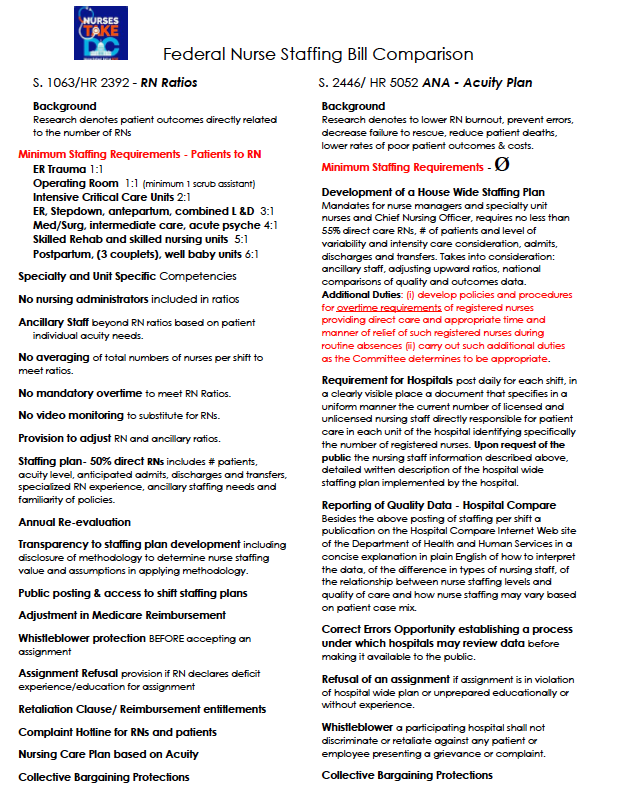
Our RN Ratio bills S. 1063/HR 2392 has the mandatory minimum nurse staffing ratios. The American Nurses Association bills S. 2446/HR 5052 share the importance that patient outcomes are directly affected by numbers of RN staff, but that is where the similarities seem to end.
Bottom line difference is in the ANA bill, no regulatory mandate that the employer to commit to a staffing plan in writing to begin any shift. Look at the Side by Side and you can always read each bill fully to get the flavor of the missing employer commitment to staff even though they agree fully with the research as we do: adequate numbers of nurses and support staff provides the patient with better outcomes.
Visit nursestakedc for information on the movement #NursesTakeC
Specializes in Nurse Leader specializing in Labor & Delivery.
SC_RNDude said:
With mandated ratios, the bedside nurse wouldn't have any say either. They are going to get the max allowed, regardless of the complexity and need of the patients.
Exactly. Which is why it's important to staff based on acuity, not nurse/patient ratios.
On my unit alone, we could have 6 patients and need 1 nurse, or 6 nurses.
Who actually read the ANA's position on this? Where do you disagree?
Quote
To explore the clinical case for the effect of nurse staffing models, we collaborated with health care insight leaders Avalere and a panel of top nurse researchers, thought leaders and managers. The white paper concludes that staffing levels in a value-based health care system should not be fixed, as day-to-day hospital requirements are constantly in flux.
With mandated ratios, the bedside nurse wouldn't have any say either. They are going to get the max allowed, regardless of the complexity and need of the patients.
That's not my experience in our ICUs. We do have mandate ratios, of course, here in California. But often times, the nurses in our ICUs are singled because the patients are too "busy" to permit the nurse to effectively care for a second patient.
That's not my experience in our ICUs. We do have mandate ratios, of course, here in California. But often times, the nurses in our ICUs are singled because the patients are too "busy" to permit the nurse to effectively care for a second patient.
Fair enough. There are places like yours, and mine, that don't need mandated ratios.
What those places do is more in line with the bill that the ANA is supporting.
Who actually read the ANA's position on this? Where do you disagree?
I agree that workload based staffing requirements would be better than simple ratios, but the ANA doesn't require that either. The ANA proposal at the federal level is the same as what they've backed at the state level, which is generally worthless. It only required that facilities create a safe staffing committee, the committee comes up with staffing recommendations, which the facility is then completely free to outright ignore.
Specializes in ICU, Cath Lab/IR CCRN. SRNA Class 2026.
I don't know how much more clear it can be made with the post that the bill for mandated ratios actually includes acuity. Read the part about acuity. SMH... Anyone who works in facilities that actually follow their staffing committees recommendations should feel very lucky and understand thats not the case for many nurses across the US.
Specializes in ICU, Cath Lab/IR CCRN. SRNA Class 2026.
The ANA legislation is worthless in a lot of hospitals as management staffs from a budget and census. Not necessarily acuity. The benefit of having ratios is that it "sets a limit" to the number of patients a nurse must take. It includes acuity so the "acuity" argument against the bills HR 2392 and S 1063 is invalid. Ever vacation out of state? Don't get sick because you never know what crap shoot you will get. Especially in desirable destination states like FL. It is tiring seeing acuity be used as an excuse not to support the ratio bill. Nurses can ALWAYS be given less patients.
Specializes in ICU, Cath Lab/IR CCRN. SRNA Class 2026.
Their legislation looks great on paper. Problem is... many states who have acuity based legislation are still struggling with unsafe ratios and working on getting ratios because of it. For example... Ohio, they have the ANA state legislation, ICU nurses are reporting getting 3/4 critical (multiple critical drips, ventilated, and unstable patients. I have seen the same testimonies in Illinois (who also has ANA legislation). The legislation has no real teeth to hold hospitals accountable. It is legislation that caters to hospital administration with an attempt to make nurses feel involved in the process. The verbiage appears as though the bedside nurses will ACTUALLY have a voice which in reality is often over ridden by management. We need a set limit to the amount of patients a nurse is forced to take. Ratio legislation is great because we can have the set limit and still adjust down in patient assignment for acuity.
You can believe that the ANA bill isn't all it might look like on the surface by noting who approves of it.
A staffing committee without a few more guidelines is problematic, period.
Certain people are invited to be on the committee. If a few reasonable and prudent nurses are invited to participate they invariably come back and report what they tried to discuss and how eventually it came around to the fact that whatever decisions they were supposed to be participating in were actually already made. This is not a "sometimes" thing; it is expected standard operations.
There is, and always has been the option of an organization doing what is ethical based on their own volition. Those who have been responsible in the past may handle a flexible plan responsibly in the future. But isn't this whole issue because of those who already haven't done just that? So how does one argue for flexibility when flexibility has always been an option and hasn't been utilized responsibily?
(I don't like the idea of mandated ratios and IMO neither one of these are worth the paper they're written on; I'm just arguing against the insanity of the idea that hospitals will use the concept of flexibility in an ethical manner).
By the way:
Quote
"(f) Refusal Of Assignment.
-A nurse may refuse to accept an assignment as a nurse in a participating hospital, or in a unit of a participating hospital, if-
"(1) the assignment is in violation of the hospital-wide staffing plan for nursing services implemented pursuant to subsection (a); or
"(2) the nurse is not prepared by education, training, or experience to fulfill the assignment without compromising the safety of any patient or jeopardizing the license of the nurse
There is no way this will play out the way a casual reader might imagine. And the fact that they used the wording "....or jeopardizing the license of the nurse" should be considered with maximum suspicion, IMO. Maximum. Anyone who reads much on this forum knows why I say that.

klone, MSN, RN
14,857 Posts
Exactly. Which is why it's important to staff based on acuity, not nurse/patient ratios.
On my unit alone, we could have 6 patients and need 1 nurse, or 6 nurses.