***Some things are specific to the speciality but I want a general nurse reply as it can happened anywhere! Thanks.***
Please tell me I'm not the crazy one!
I work have worked in the NICU for about 3 years. Over the years, I have noticed some nurses on the opposing shift are a bit feisty but I have gotten over it for the most part. BUT, this small stupid thing has put me in a tizzy (sp?), and I more so need to vent than anything, but all are welcome to input your little "over-the-edge" incidences and what you do in response/to get over it.
So to the point. I was having a really fantastic day; all my babies were cooperative, all quietly snuggled back in, parents all had a good (as good as it can get) day. It was not crazy admit day or let's make a bunch of changes day - IT WAS A GOOD DAY! It was nearing the end of my shift and as I almost always do unless we are slammed, I made the haul to restock all of my patients' supplies, any and everything they would need for the next 2 shifts.
Shift change happens and I give report on my first two babies and I come to my third who is a different nurse taking them. I start my report as always, name, parents, etc. After the whole introduction, I casually skipped to the respiratory support. In the middle of saying, "I have only titrated my Os between 24% an--" the nurse butts in, holds up her hand and says, "Please,... (*hand to a fist now*) what's the patient's history?" Me: Uhhhh, PTL.
THAT WAS IT... PTL. You know, I thought about it, and yea, maybe I should have said PTL before jumping right into the whole gaggle. Maybe I should have also added the 3 weeks old apgar scores and the whole resuscitation efforts. Maybe I should have gone through the whole pregnancy timeline.
I know, I'm going too far but it kinda irked me. Yes, if there is a significant amount of history, I will start with that. But seeing as it was such a short and kinda insignificant history, it slipped my mind this time. (Serious on the apgar scores, I'm not telling you 3 week old apgar scores unless it's like 0,0,2,4,5,7)
And to be honest, I would not even mind to have stopped right there to say the history had it not been asked of me in a completely ******* rude way and tone. Honestly, I would have even given an, "Opps, sorry."
I just don't get it. What makes people behave like this after not even being somewhere for 5 minutes. I get you have a life, but don't treat people like scum of the earth just because your mind cannot get over having respiratory before history. Like, MY GOD, sorry I ruined your day...
Sorry, I know I took a mole hill and turned it into a mountain. I get that. What I don't get is how people lack a decent sense of manners.
Thanks for reading. But please do leave your experiences NICU and non-NICU. These situations happen everywhere, so even if you have them, say your non-nursing related stories too. I like to read on your guys experiences which far outweigh mine!
Specializes in Surgical, Home Infusions, HVU, PCU, Neuro.
Well his took me so much longer to read than it should have! Dear Google was having me "praise the lord" and that had me all mixed up lol. The diverse personalities we encounter each and every day certainly keeps us on our toes, whether it is coworkers or patients and/or family. How I was trained as a New Grad I'm sure is completely different than anyone else, and by the time I took and manipulated everyone's "brains" and perfected my own, I'm in my own class now. I have my highlighters ( each color is assigned to it's own meaning) and at least 2 color pens ( one for report in the beginning and a new color for changes throughout the day) and this is me, each and every workday. I would like to say I'm some what lax with report, but I'm sure someone would say differently. If my patient is an EMU pt, I am usually not concerned when the last BM was, but if my pt is in with PNA a history of COPD and has only had supplemental oxygen this admission, there is more relevance for this info. If a pt is admitted with Crohn's exacerbation and had a GLF before admission, the fall is relevant until ruled out ( true experience pt admitted during the night had CT ordered the morning I was there, radiology calls, massive brain bleed, sat on the pt for 6 hours before an ICU bed available, where neurosurgery was in the room before the pt to do a ventric drain)
Ive had nurses come in and go through the pt assigned to them chart and write everything down, nurses quiz me in report about different tests and results ect and bring it to management if something wasn't known. Exhausting.......
I do understand the frustration on how the information "requested" and that might rub me the wrong way too. I have absolutely no clue on NICU (except to give all that works there mad props!) and your relief would not have been happy if I was the one giving report, ( although I was praising the Lord!)
Most of the nurses on my unit (adult ICU) use the same report sheet, and most of us try to go in order so we don't leave things out. However, all the demographic stuff is at the top (proxy, code status) and also precautions (Contact, aspiration). Right there, it's easy to get sidetracked ("he's a DNI, so after he desatted last night they tried a Venturi mask but now he's on bipap and he originally desatted because he was trying to eat his pureed diet but because of his previous stroke he has left-side weakness and swallowing difficulties and he might have aspirated and also hasn't had a BM in 4 days so we put in an NG tube which is to suction now but still needs x-ray confirmation before he can get meds....) You get the idea! Some of my coworkers get noticeably ruffled if I skip over a category & come back to it. Others 'go with it' and jump around the sheet to fill things in. *I* think I usually get the full story out if they pause a second and let me complete the scenario. Probably some of them, on some days, think I should just go system by system.
Yes indeed it happens everywhere! It is not the place it occurs it is merely the person and their attitude toward life! The person is more than likely the same no matter who they are dealing with.
I understand. When I was a new nurse and in orientation yet I had a nurse who was an / asshat. I never had any issues with any of the others. Found out she was going through some difficult personal situations. Although it didn't excuse her from taking out her frustration on me, I understood why she was that way.
Wow. That was kind of nasty. Sorry OP: you are a human being first and foremost - you deserve to be treated with respect and dignity. Always. Just like everyone else.
I've discovered - after having lived hundreds and hundreds of years (LOL) - that some people are just vile right down to their core. Even if they bother to try to hide it, it eventually slops over into other aspects of their lives at inappropriate times. It's not a question of if - more like a question of when. Unfortunately, work is common place for this to happen (much to the dismay of the coworkers working with this type of person).
Then again, there are those whom just don't give a rat's orifice what other people think about them. I find that type of person mentally exhausting, because they rain their dark mood and negative energy all over the place - inflicting it on others, or seeming to take sadistic pleasure in just being as unpleasant as possible. That gets old after a while, and I find it's draining too because I tend to try to shield myself like crazy when in the company of the chronically angry.
Some people just have short fuses (NOT an excuse) and are similar to a powder keg of gunpowder just waiting for the tiniest of sparks to ignite (((Houston, you are cleared for blast off in T-minus 10 seconds … 9 … 8 … )))
CABOOM!!!
Taking into account the scenario you described, you likely would have been a target for her anger for some minor offense (any it seems will suffice) before you got through report, whether you gave her all the information in the precise order she felt necessary, or not. It seems her intent was to belittle and upset you for her own personal reasons: mission accomplished.
I find it interesting that people whom are chronically angry, and lash out randomly at others will usually get extremely upset when they get a dose of their own medicine. You'd think if they can dish it out that they could take it pretty well too - not the case in my experience.
I wish I had a magic formula for you to be able to counteract future histrionics and drama with this coworker, but if there is an effective way to do it without it escalating into something confrontational I sure don't know about it.
I do want to ask since you brought up SBAR. I know it is a communication tool and some might even say "report" tool but do you think SBAR is an efficient handoff tool? I have heard before that the format of a SBAR doesn't quite equal a nurse to nurse handoff. It is more of a tool of communication between physician and nurse.
SBAR can actually be used in nurse to nurse communication effectively.
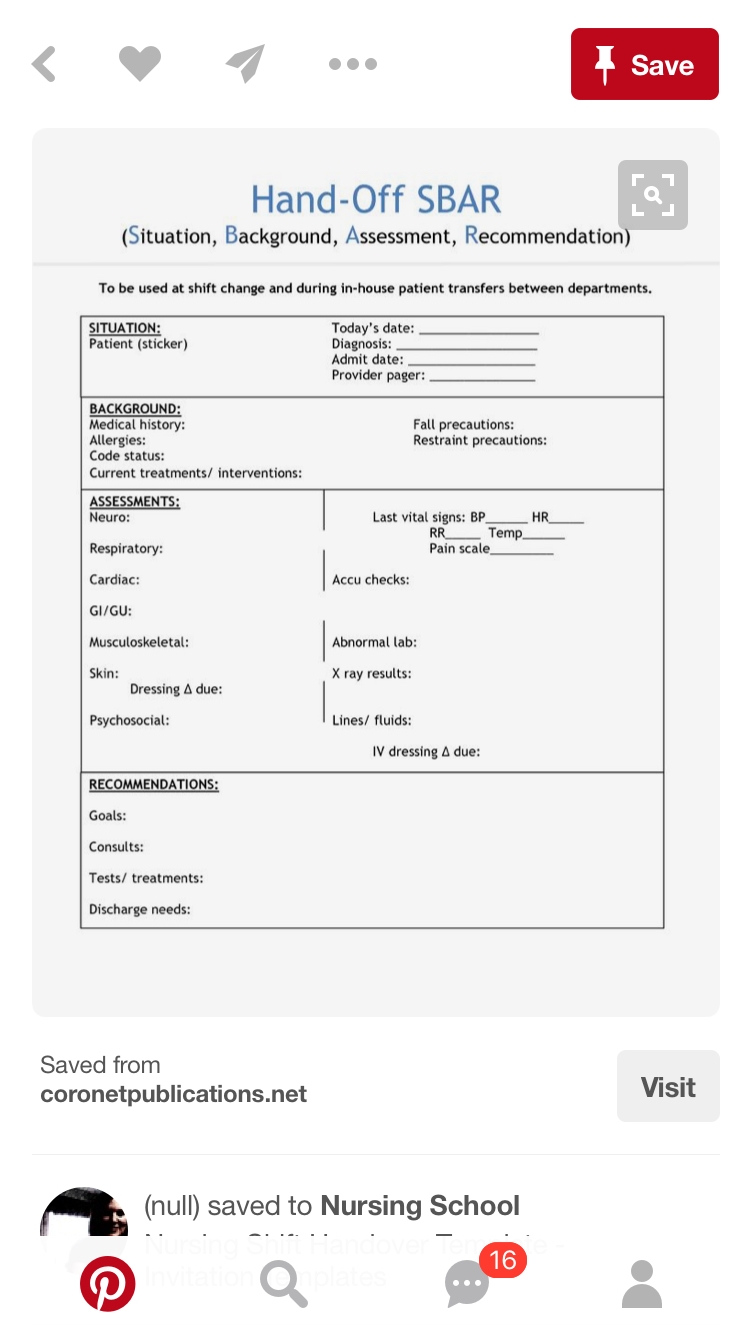
Example of SBAR template I have used in various setting of my career that I was able to find on Pinterest:
Situation: Reason baby is in NICU
Background: that would present, in your case baby was pre-term ex 30 weeker, no underlying etymology...
Assessment: the assessment of systems, social issues.
Recommendations: the POC, any changes and issues raised.
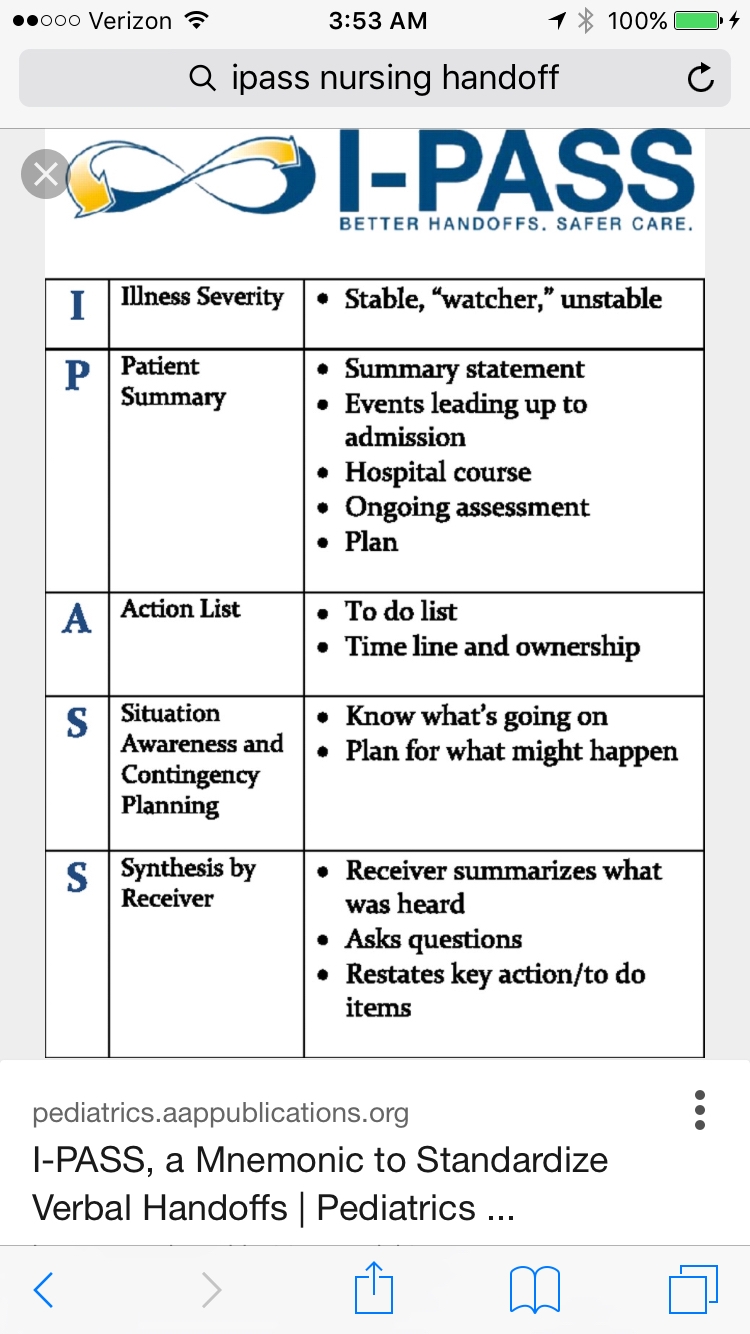
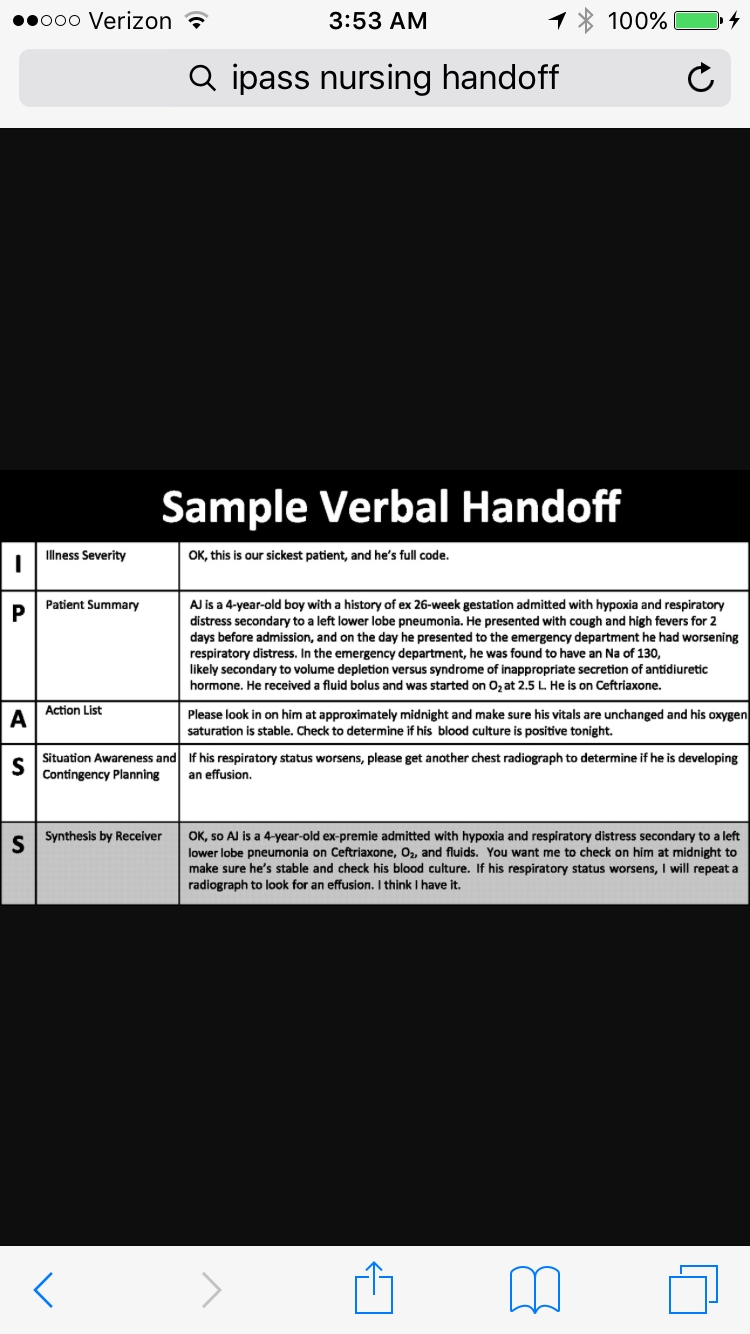
Handoff should be considered and clear; recently there have been changes in how we do report in terms of using the I-PASS method, which physicians and nurses use at may facility, which is an enhanced version of SBAR, it is straightforward and helps with assuming care.
That's why SBAR is important, and why the parts of SBAR are in the order they're in. It's hard to put current situation into context without background. Background could be as simple as "previous 28-week delivery 2/2 preterm labor." But that needs to come at the beginning of the report, not after all the minutia of vent settings, I&O, etc. And it doesn't have to be long and detailed with pregnancy hx and all the resuscitation efforts. Short and sweet, such as what I said above.
And yes, you are making a mountain out of a molehill. If you let THAT one comment ruin or shadow a previously great day, well....you shouldn't.
Agree. We all have brains that work differently as far as processing information. There are reasons we have structures in place for report to guide us. However....rudenes isn't ever good. IF, I feel I need a piece of information that has been skipped, in order to process the information, especially a patient I am not familiar with, I might...might, interrupt and politely ask the question. Often I apologize, and say, I am sorry to interrupt you, what was the "XYZ?". Plenty have been irritated by even this. My point is that we all need to work together and sometimes the assignments are so heavy, that to comb through a chart to find out what you want to know takes a bit of time. If I can ask you and get the answer in 1 second, then I feel I am being efficient. IF what I am asking has a complicated answer, then that is a different subject.
On the other side, I have NO PROBLEM stopping to clarify for the one I am giving report to. What's the big deal? Work with each other. We all have different needs, levels of knowledge etc...I have given report on complex...truly complex patients in PICU where the on-coming nurse doesn't write down one thing. Doesn't bother me. I Envy their ability to carry on that way. I just don't function that way. I wouldn't insist they write everything if that is not what they need. Work with each other And respect the fact that we are all different in how we process information. I know there have been some who consider me a pain in the butt. I also know of plenty of others who appreciate the way I give and receive report.
SBAR can actually be used in nurse to nurse communication effectively.
Example of SBAR template I have used in various setting of my career that I was able to find on Pinterest:
[ATTACH]22721[/ATTACH]
Situation: Reason baby is in NICU
Background: that would present, in your case baby was pre-term ex 30 weeker, no underlying etymology...
Assessment: the assessment of systems, social issues.
Recommendations: the POC, any changes and issues raised.
Handoff should be considered and clear; recently there have been changes in how we do report in terms of using the I-PASS method, which physicians and nurses use at may facility, which is an enhanced version of SBAR, it is straightforward and helps with assuming care.
Great information.....thanks for the reference....
SBAR, Systems report..... Different units/specialties usually have a particular method of report that is consistently used on a particular unit. The nurses who work there become accustomed to the information given in a certain way. Not ALLWAYS necessary to include every detail depending on the patient, so to say something like "nothing out of the ordinary with X, or Y within normal limits" is fine with me as long as it is addressed.
Specializes in Huntingtons, LTC, Ortho, Acute Care.
There Will always be nurses that are *hem hem* anal. I have a couple on my day shift that are like that and I HATE doing report with them. There are nurses you can do report within 10 minutes clean your mess and head for home, then there are nurses that take you till 7:30 or more cause they want it all.
I have reminded these nurses on several occasions, "I only report the meat and potatoes, and if I don't relay something important to you, it is because it was not relayed to me. I too have responsibilities I need to tend to over night"
no I probably am not aware of the fact it was bone on bone pre joint replacement and their DJD diagnosis was over 10 years old... But that also doesn't save their lives in an emergency... But the surgery they had, who the surgeon and attending is, last set of vitals, last time medicated with PRNs and what it was as well as dose, their progress with therapy, any specifics (crush meds, aspiration precaution, no BP in L/R arm, due to void). Maybe I should be more descriptive, but I just don't have the time or desire to explore the chart, so long as they are stable and I have the meat and potatoes I'm happy! And sorry but what rehab, ALF, or home
health agency the patient will be discharge with doesn't matter to me! And can easily be found by you when you're ready to discharge or call report over, there are no case managers at night so a patients discharge is far from my mind.
everyone is different, and everyone finds different pieces of info important. The only thing I can really suggest is to just breath through the rudeness, and Spanish Inquisition of a report, tell them what you know. if you don't know it offer to look it up but remind them they can look it up for themselves too. In intensive care especially things can change by the minute! Some hills are just not worth dying on.
If you feel so strongly about this I would ask coworkers how they feel about giving report with this nurse. If you're the only person with a problem maybe it be best to request your charge nurse not assign you to patients she has had. And explain why you would rather not have hand off with her. If it is multiple nurses that get issues from her band together and direct this to your manager, everyone has a right to be respected, and there's ways to ask for the info you seek without being rude. She may need a reminder about this from her boss, she may not even be aware of the fact she comes across as ******!


Kallie3006, ADN
389 Posts
Well his took me so much longer to read than it should have! Dear Google was having me "praise the lord" and that had me all mixed up lol. The diverse personalities we encounter each and every day certainly keeps us on our toes, whether it is coworkers or patients and/or family. How I was trained as a New Grad I'm sure is completely different than anyone else, and by the time I took and manipulated everyone's "brains" and perfected my own, I'm in my own class now. I have my highlighters ( each color is assigned to it's own meaning) and at least 2 color pens ( one for report in the beginning and a new color for changes throughout the day) and this is me, each and every workday. I would like to say I'm some what lax with report, but I'm sure someone would say differently. If my patient is an EMU pt, I am usually not concerned when the last BM was, but if my pt is in with PNA a history of COPD and has only had supplemental oxygen this admission, there is more relevance for this info. If a pt is admitted with Crohn's exacerbation and had a GLF before admission, the fall is relevant until ruled out ( true experience pt admitted during the night had CT ordered the morning I was there, radiology calls, massive brain bleed, sat on the pt for 6 hours before an ICU bed available, where neurosurgery was in the room before the pt to do a ventric drain)
Ive had nurses come in and go through the pt assigned to them chart and write everything down, nurses quiz me in report about different tests and results ect and bring it to management if something wasn't known. Exhausting.......
I do understand the frustration on how the information "requested" and that might rub me the wrong way too. I have absolutely no clue on NICU (except to give all that works there mad props!) and your relief would not have been happy if I was the one giving report, ( although I was praising the Lord!)