I'm a senior nursing student and this debate arose with a couple of my classmates and me. I work as an ER tech and they work as patient care techs on the floor. As of right now, CDC guidelines state for PPE:
Quote
Updated PPE recommendations for the care of patients with known or suspected COVID-19:
Based on local and regional situational analysis of PPE supplies, facemasks are an acceptable alternative when the supply chain of respirators cannot meet the demand. During this time, available respirators should be prioritized for procedures that are likely to generate respiratory aerosols, which would pose the highest exposure risk to HCP.
Facemasks protect the wearer from splashes and sprays.
Respirators, which filter inspired air, offer respiratory protection.
When the supply chain is restored, facilities with a respiratory protection program should return to use of respirators for patients with known or suspected COVID-19. Facilities that do not currently have a respiratory protection program, but care for patients infected with pathogens for which a respirator is recommended, should implement a respiratory protection program.
Eye protection, gown, and gloves continue to be recommended
So basically CDC is saying wear an N95 if you have it, but if you don't, wear a surgical mask until you can get an N95.
So if you have a suspected or confirmed COVID-19 patient, and all you have is a surgical mask and no N95, can you refuse to take care of that patient? Do you face any legal repercussions or potential fallout from your employer if you do refuse? Asking not only about tech positions, but RN positions as well.
Non-healthcare workers aren't going in and out of high-risk Covid 19 pt populations for 12-13 hours a day either. I am on a Covid-19 unit for a large hospital. I am 3 to 1 with telemetry and step-down Covid high-risk pt's, it is a huge undertaking. I am told soon we will have to take 4 pts, some stepdown and some telemetry, Our doors are not glass-enclosed, you cannot see the pt. 's.
The donning and doffing are encumbered by disorganization, lack of various supplies at any given time and how to attain them when you do run out. There's confusing Covid updating, some of us have been educated via a training class, others have not. Our techs are disappearing, so I am doing everything from toileting, bathing, linen changes, getting glucose checks and VS's to my regular duties of care. I am exhausted. I will give notice if they go 4 to 1, with high acuity and high-risk conditions for the same patients.
I signed on to care for others with the right skills, training, and equipment. I have been an American Red Cross volunteer as well for years.
I think we should have a voice and some rights when it comes to being on the frontlines of a Pandemic. I know MunoRN will have an issue with this, frankly, I don't care. You sound like admin, not like a current
Covid 19 bedside nurse. Just sayin..
Admin, ouch.
I'm actually a bedside nurse, I've been caring for Covid patients since the end of February.
I'm not really clear what you took offense with, the post you quoted was in response to a question of why ideally non-covid patients might be given to immunocompromised and older nurses given their significantly increased mortality risk with covid. It was then questioned whether older and immunocompromised healthcare workers really had a higher mortality risk or if that was just true for non healthcare workers, thus the response you quoted.
I'm well aware of the chaos and absurd workloads of working in a Covid-slammed hospital, I've been doing it for the last month.
I've also pointed out on a few occasions that administrators and others have been pushing to have us work in avoidable unsafe conditions, so I'm at a loss about what you're referring to.
Suspected COVID patients at our hospital and confirmed cases are not taking care of anyone else. The alternative is to let the patient die if we don't take care of them.
Equipment is never, ever guaranteed. I have written a letter to my BON that full action should be taken against any nurse that refuses to care for a patient....IF A SHORTAGE SHOULD OCCUR.
WOW! that is cruel and crude,shows your compassionate side,you are not really a bedside nurse are you? Eating any young lately? ......
50 years ago I was a young medic in Vietnam. We had to do so scary stuff but we were never ordered into battle without ammunition. For some of us, sometimes the ammunition ran out. When that happened they died. They were soldiers and they didn't have any other choice. No nurse gets paid enough to die for her patients.
Refusal on these grounds isn't justified in my State (Pennsylvania) or my hospital network (redacted for job protection) because they both have adopted the CDC guidelines for patient care, which is that surgical masks are sufficient outside of aerosol-generating procedures.
There are a couple of things at play here. One is that nobody actually knows enough about this virus to say for sure how its transmitted or what proper precaution is. We want to err on the side of self-preservation, the hospitals want to make it as easy as possible for as many people as possible to be "protected." And in the middle is the very real reality that there needs to be some understanding by everybody that there aren't enough N95s to go around right now and we have to be a little smart.
That aside, because the state boards of nursing and hospitals are in compliance with surgical masks, you don't have any recourse of refusal absent N95s. It sucks, but that's how it is. They aren't even making concessions for pregnant providers. It's a wild world right now.
If you take care of a patient without appropriate PPE, you risk contracting the virus and taking it to the rest of your patients for 2-14 days until you realize you are sick, as well as family members, grocery store clerks, etc. You could kill several people accepting an unsafe assignment. Don't do it.
I'm a senior nursing student and this debate arose with a couple of my classmates and me. I work as an ER tech and they work as patient care techs on the floor. As of right now, CDC guidelines state for PPE:
So basically CDC is saying wear an N95 if you have it, but if you don't, wear a surgical mask until you can get an N95.
So if you have a suspected or confirmed COVID-19 patient, and all you have is a surgical mask and no N95, can you refuse to take care of that patient? Do you face any legal repercussions or potential fallout from your employer if you do refuse? Asking not only about tech positions, but RN positions as well.
If you are very worried, is it possible to take a hiatus until things return to usual? I think this is the part pf bedside nursing, nurses may not like,
Specializes in Former NP now Internal medicine PGY-3.
long story short if the hospital is following current CDC guidelines then I doubt anyone will get away with refusal. Whether or not the CDC is sure on his and how much data there is backing it doesn’t matter unfortunately.
But I will say there are very few airborne diseases most being droplet. Of course minus certain procedures.
There would likely be employment repercussions, to include termination. In some states, there may even be Board repercussions.
Ultimately, we each get to make our own decisions and weigh the risks in our free society though. Nobody can force nurses to physically present to their assigned units when scheduled and provide 12 hours of competent nursing care without appropriate PPE. Forced labor is illegal in this country, so there's really nothing we need to "get away with." Failure to work a scheduled shift is not abandonment, nor criminal.
since community spread has happened all across the US, and testing has been slow to get to hospitals and states... It is clear, any RN providing "any" patient care should have at least an N95 mask. Surgical masks are not protective enough, and still there are many "unknowns" about COVID-19.
The facts are that many Italian RNs and Medical providers have contracted the disease and now we will wait and watch our own in the US do the same?
This to me is unethical, unacceptable, and wrong. Something must change NOW.
If an Employer makes a decision to terminate someone with ethical principles, and a desire to not spread the disease to anyone else...then they are truly unethical and should be ashamed. Any nursing board that judges empathetic caring nurses making smart decision to not work under these conditions is WRONG. We have to stand by our standards of care, the importance of patient safety and the importance of not spreading infectious disease no matter if it means less RNs or providers per patient - until the proper PPE is available to all PERIOD.
long story short if the hospital is following current CDC guidelines then I doubt anyone will get away with refusal. Whether or not the CDC is sure on his and how much data there is backing it doesn’t matter unfortunately.
But I will say there are very few airborne diseases most being droplet. Of course minus certain procedures.
CDC guidelines are for N95 or 100 level protection, some states and hospitals have opted to instead go with surgical mask protection. The level of protection these provide is not really known since they aren't intended for that purpose and therefore aren't tested for wearer protection performance. Some studies have been done and find that these masks typically filter about half the inhaled air, which in the case of a virus is basically pointless.
As far as limiting more effective airway protection to certain procedures there is absolutely no evidence these procedures produce significantly more virulent droplets than a cough does, and these patient are almost always coughers.
I think there's been confusion about the level of respiratory protection required to protect the wearer from droplet transmission, not just airborne. For viruses, where reducing the amount of inhaled pathogens, rather than full protection, is basically useless, N95s are arguably insufficient, N100 (HEPA) is really the only worthwhile protection.
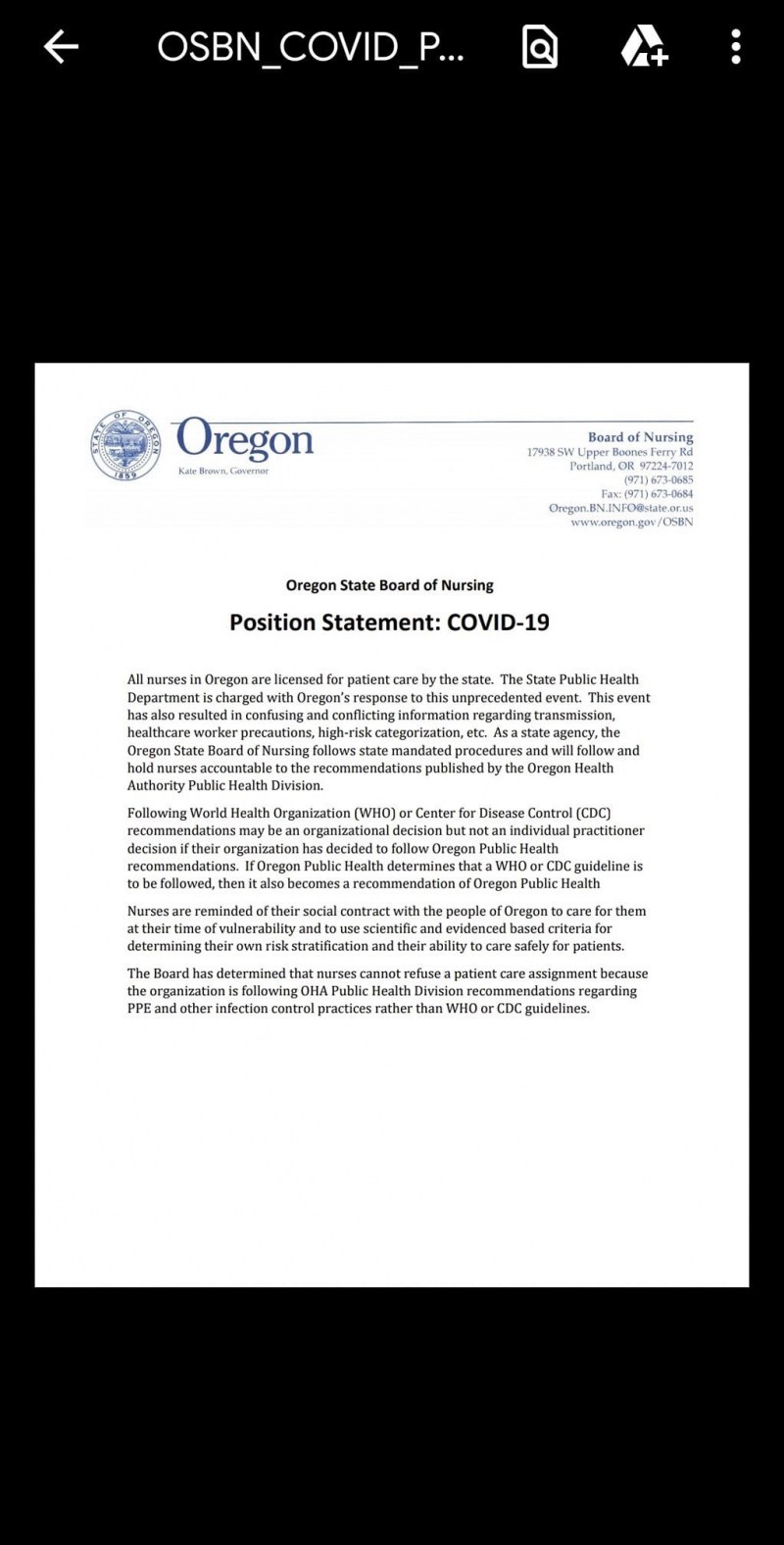
Does anyone have a credible reference to support that any state's BON would take action against a nurse who refused to work because of lack of appropriate PPE? I don't mean they might, or they could, or my cousin said her co-worker. I mean a source from a Nurse Practice Act or your state's BON regulations.
Does anyone have a credible reference to support that any state's BON would take action against a nurse who refused to work because of lack of appropriate PPE? I don't mean they might, or they could, or my cousin said her co-worker. I mean a source from a Nurse Practice Act or your state's BON regulations.
ZThe "scientific and evidence based criteria" they're referring to is neither of those things. The state's criteria is that procedure masks is sufficient protection.


 The "scientific and evidence based criteria" they're referring to is neither of those things. The state's criteria is that procedure masks is sufficient protection.
The "scientific and evidence based criteria" they're referring to is neither of those things. The state's criteria is that procedure masks is sufficient protection.
MunoRN, RN
8,058 Posts
Admin, ouch.
I'm actually a bedside nurse, I've been caring for Covid patients since the end of February.
I'm not really clear what you took offense with, the post you quoted was in response to a question of why ideally non-covid patients might be given to immunocompromised and older nurses given their significantly increased mortality risk with covid. It was then questioned whether older and immunocompromised healthcare workers really had a higher mortality risk or if that was just true for non healthcare workers, thus the response you quoted.
I'm well aware of the chaos and absurd workloads of working in a Covid-slammed hospital, I've been doing it for the last month.
I've also pointed out on a few occasions that administrators and others have been pushing to have us work in avoidable unsafe conditions, so I'm at a loss about what you're referring to.