I apologize if this has already being posted, I'm days old in this forum...
Pain Scales are used by us constantly, Pediatric Emergency/Trauma Center, yet we get those flat affect, normal vitals, stating they are in a 10 out of 10 pain.
pain is whatever you say it is, but I'm also going to note all the various actions that paint a factual picture of how well you handle that pain...
I'm sure someone here has already posted Hyperbole & a half's pain scale, but I just love it so... and since it's original posting I've used 'being mauled by a bear' when explaining the scale to some.
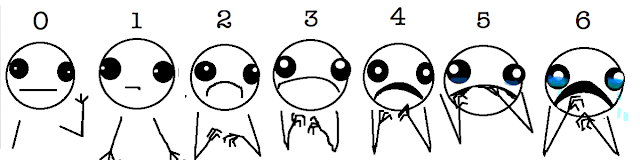
Brosh's interpretation of the Wong Baker scale:::
0: Haha! I'm not wearing any pants!
2:Awesome! Someone just offered me a free hot dog!
4: Huh. I never knew that about giraffes.
6: I'm sorry about your cat, but can we talk about something else now? I'm bored.
8: The ice cream I bought barely has any cookie dough chunks in it. This is not what I expected and I am disappointed.
10:You hurt my feelings and now I'm crying!
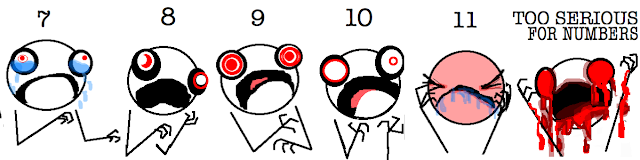
Brosh's explanation of the more extreme Pain Scale is as follows:::
0: Hi. I am not experiencing any pain at all. I don't know why I'm even here.
1: I am completely unsure whether I am experiencing pain or itching or maybe I just have a bad taste in my mouth.
2: I probably just need a Band Aid.
3: This is distressing. I don't want this to be happening to me at all.
4: My pain is not f*ck!ng around.
5:Why is this happening to me??
6:Ow. Okay, my pain is super legit now.
7: I see Jesus coming for me and I'm scared.
8: I am experiencing a disturbing amount of pain. I might actually be dying. Please help.
9: I am almost definitely dying.
10: I am actively being mauled by a bear.
11: Blood is going to explode out of my face at any moment.
Too Serious For Numbers: You probably have ebola. It appears that you may also be suffering from Stigmata and/or pinkeye.
curious what other's do w/ the cool calm and collected who may or may not be actively eating McDonald's, or who may or may not be crushing candy, or playing xbox in the waiting room...
I've always hated the scale of 0-10 method of rating pain...although your creative post gave it some much needed clarity:-)
When documenting an assessment we should include the subjective and objective data. We should be to the point and not try to downplay what the pain may be based on the presentation. This has a lot of cultural aspects as well as a person's own way of dealing with pain. My husband will scream if someone steps on his foot. I actually waited a year to go to the doctor to find out that mine was broken. We all experience pain differently and express a different reaction to feeling the pain. Two people could have the same injury and one can be screaming bloody murder and the other person could be sitting there stone faced. They may be hurting just as much, they just aren't the type to scream about it...I will say that the munching on fast food and playing XBOX with a 10 out of 10 is a little over the top though....I just can't stand the 0-10 scale, especially if it's an intermittent type of pain that can be fine one minute (usually when the doctor comes in the exam room) and excruciating the next (out of nowhere, waking the patient up from a sound sleep).
What I did was this, treat the pain with what the doctor ordered. If they are still complaining call the doctor and relay all subjective and objective data and see what the doctor wants to do to proceed. This way, you've covered yourself and cannot be accused of leaving a patient in pain and failing to call the MD.
Subjective and objective findings are the part of any good assessment.
FWIW, in my ER, a pt's pain rating doesn't have much effect on their treatment. The docs don't read them.
If we actually gave narcotics based on numerical pain scores, and word got out, we would have to hire a whole lot more staff.
(my bold)
Are there any other signs or symptoms that are habitually ignored by the physicians or is it limited to the patient's report of pain? Even if the doctors neglect this part I'm sure that you'll advocate for your patients?
If it's true as you say that the patient's report of pain rarely affects the treatment they receive, aren't you concerned that a lot of patients might not be adequately treated and as a consequence suffer needlessly?
curious what other's do w/ the cool calm and collected who may or may not be actively eating McDonald's, or who may or may not be crushing candy, or playing xbox in the waiting room...
I just document the pain score that they tell me along with my objective observations and move on. I also ask about the quality of the pain, whether it is constant or intermittent, if there is anything that makes it better or worse, and if they have taken any medications to address it.
Here is how I deal with it...I don't ask the patient to rate their pain. They ask for pain meds and I give it! Here is why...Patient X ask for pain medicine, being the awesome nurse that I am I ask patient to rate their pain on a scale of 0-10. Patient X says his/her pain is currently a 2. VSS and no other obvious signs of distress. Guess what I do and all of you do too....You get the patient the med! If you dont, well you all know about those all important patient satisfaction scores lol
When I go patient room, I always asses their pain. Where I Work; I have to document Q4 hour pain. If they ask pain meds yes I give. I don't give med just because he told me his pain 8, I give because he request it. However of course I do document . Even when they sleep, we have to document as non verbal pain assessment.
One of the things that we encouraged over the past 10 years was for patients to be pain free- setting the expectation. For some people- myself included- one might never be pain free... If the promise of being pain free is there one might focus on the pain, and by doing so make the pain worse....
If a patient states in a calm manner their pain is 10 I try to educate them as a phone triage nurse that I would be at the ER already if my pain was that high.
I do dislike that people that are on chronic opiate medications state "I have a high pain tolerance, so my pain is worse than other peoples"- I just state that the number is subjective to let us know if their pain is increasing or decreasing.
Pain is an area that needs comprehensive management- it should not be left up to the patient to figure out how best to control the pain- however if they have a reasonable plan/medication regiment we should listen (I also hate when I see a person who takes two percocet a day for multiples of years to be told by the MD that they need to find another way to control their pain...)
One of the things that we encouraged over the past 10 years was for patients to be pain free- setting the expectation. For some people- myself included- one might never be pain free... If the promise of being pain free is there one might focus on the pain, and by doing so make the pain worse....
If a patient states in a calm manner their pain is 10 I try to educate them as a phone triage nurse that I would be at the ER already if my pain was that high.
I do dislike that people that are on chronic opiate medications state "I have a high pain tolerance, so my pain is worse than other peoples"- I just state that the number is subjective to let us know if their pain is increasing or decreasing.
Pain is an area that needs comprehensive management- it should not be left up to the patient to figure out how best to control the pain- however if they have a reasonable plan/medication regiment we should listen (I also hate when I see a person who takes two percocet a day for multiples of years to be told by the MD that they need to find another way to control their pain...)
I agree. Pain is a complex problem that requires complex management. I will believe your subjective rating, but that doesn't mean I have the words Dilaudid dispenser stamped on my forehead or that I am going to slam you with a bunch IVP narcotics because that's what you say will work (this depends on the home regimen and physician's orders, of course). We have an acute pain service at my hospital, and I'll be happy to consult them.
During my initial assessments I always look for a grimace when doing deep palpation of the abd. Pts may have abdominal discomfort but unable to rate it on a numerical scale, so stimulating a grimace gives me a better idea of the discomfort/level of pain. Non verbal clues are important and reliable!!!


NurseSpeedy, ADN, LPN, RN
1,599 Posts
I've always hated the scale of 0-10 method of rating pain...although your creative post gave it some much needed clarity:-)
When documenting an assessment we should include the subjective and objective data. We should be to the point and not try to downplay what the pain may be based on the presentation. This has a lot of cultural aspects as well as a person's own way of dealing with pain. My husband will scream if someone steps on his foot. I actually waited a year to go to the doctor to find out that mine was broken. We all experience pain differently and express a different reaction to feeling the pain. Two people could have the same injury and one can be screaming bloody murder and the other person could be sitting there stone faced. They may be hurting just as much, they just aren't the type to scream about it...I will say that the munching on fast food and playing XBOX with a 10 out of 10 is a little over the top though....I just can't stand the 0-10 scale, especially if it's an intermittent type of pain that can be fine one minute (usually when the doctor comes in the exam room) and excruciating the next (out of nowhere, waking the patient up from a sound sleep).
What I did was this, treat the pain with what the doctor ordered. If they are still complaining call the doctor and relay all subjective and objective data and see what the doctor wants to do to proceed. This way, you've covered yourself and cannot be accused of leaving a patient in pain and failing to call the MD.