While on vacation outside of the US a few days ago, I had two chances to intervene in medical situations. I'm curious what you would have done if you had been in my situation.
Case 1: In a southern coastal city in the UK, an elderly woman reportedly "just fainted and fell" while crossing a street. No one there knew her. Several bystanders were trying to help, including a man who identified himself as a "medic" and woman who worked at a pharmacy. The injured woman was obese, lying awkwardly on her right hip with her torso twisted, her upper chest on the pavement and her head twisted toward her left shoulder. Her head was lower than her body, and she was bleeding from a scalp laceration. The medic knelt beside her and held pressure on the scalp wound. She denied any pain and tried to get up several times, but they held her down even when she vomited, insisting that she should not move. Her breathing was heavy. EMS had been called, and I could hear a distant siren.
Case 2: Halfway between Amsterdam and New York, they paged overhead for a doctor to come to the back of the plane. No one moved. I went back and told the flight attendant I was an ER RN, not a doctor. Apparently, I was their best option.
He took me to an elderly man who was worried about moderate swelling and mild redness in his right lower leg and ankle. With his daughter translating, I learned the swelling had started during our flight, but he'd been on a plane for three hours prior to ours. He had a large scab on his lower right lower shin from a scrape three days ago but denied any pain. He was sitting on a jump seat with his leg propped up on a window well, straight and level with his hip. They were applying cool compresses.
I've second guessed myself a bit on one of these two. What would you have done?
If you are concerned about part of the spine, you are concerned about all of it.
I think that this is what has changed and may not be clear. It seems that what they have found is injury to the spine below C1-7 is statistically unlikely in most head injury scenarios and that the current treatment (backboard+c-spine immobilization) does not meet risk-benefit standards. However, any impact hard enough to cause head injury symptoms has a higher probability of having associated cervical vertebral issues mostly due to the extreme mobility of the neck vs say the lumbar spine. I disagree that you cannot immobilize the cervical spine without immobilizing the remainder. Certainly placing a c-collar and then letting the patient walk around is useless but a c-collar and hands on or putting the patient supine on a firm (not hard) surface is adequate.
I would always offer on a plane. IMO, the best case scenario is that everyone with medical training will offer and you can discuss amongst yourselves about who is most qualified for this - and who to perhaps confer with if needed. Similar to what was mentioned in the linked article, it can get complicated as to which is the most appropriate/qualified.
an ICU RN, a cardiologist, an NNP, and a radiologist all respond to the emergency call. What is the issue? The cardiologist has had a drink or two, doesn't feel drunk. The ICU RN is a new grad just out of orientation. The NNP is experienced, but that experience is exceptionally narrow. The radiologist is not used to dealing with patients like this - she looks at a computer screen all day.
Chest pains? ICU RN for front line care with the altered cardiologist to give verbal backup and support, as long as they've disclosed their drinking and have stopped (which is why they shouldn't be hands on).
Woman delivering a baby? Radiologist and NNP. The radiologist can take care of the mom, the NNP will take care of the baby. (cardiologist and radiologist both have distant training how to do it, and the radiologist hasn't been drinking).
Seizures? ICU RN with other professionals as backup/extra hands.
Coding? Everyone except the cardiologist can help - but the ICU RN and NNP have more code experience than the radiologist (NNP's codes might be with babies, but you are in a good habit of being in that situation, less likelihood of panic/freezing)
I am not worried about being sued or getting into trouble for offering help. No jury will convict assistance offered in good faith even if someone did sue.
In a situation when I am the only person available and I may have had a drink? If I am literally the only person that can help, I will offer and tell everyone, patient, family, staff, that I have had a drink and I cannot accurately guarantee my level of impairment, but if I'm the only thing you got, I might be better than nothing. In the latter situation, my preferred situation would be to be able to give my observations to another provider who is on a phone (again, disclosing I've had a drink). There are even situations where someone could be totally sloshed and if there is no one else to help, they might still be better than inaction. (for example, if a woman delivered a mildly premature baby, the NNP could make sure they know to do kangaroo care until they can land. That she would know in her sleep. Obviously that would be incredibly terrible as a situation, but the chances of it happening are so extremely rare.
The flight attendants wouldn't automatically know who is most suited, and often if most people won't say they can help, there's no chance to know who could best help.
I do transport as an NNP and even if I was the only person available on a flight, I could at least talk to ground support to give accurate assessments and carry out recommendations. I know there is always ground support somewhere.
I also think back to the case where the woman died on a flight back from Hawaii when they didn't divert when recommended by the doc who responded. That doc made a mistake, IMO, because the first time she lost consciousness (which was written off as syncope due to anxiety, without ever having a history of syncope), the flight should have landed ASAP. It was over an hour later when she had the loss of consciousness with loss of bowel control/seizure. But no one is getting upset at him (likely helped by the fact they were over water with nowhere to land anyway). Even with the mistake, it was given in good faith, and there weren't other people giving other options or disagreeing.
Lots of rambling to say, legal consequences be damned, the moral and ethical thing to do IMO is to offer aid.
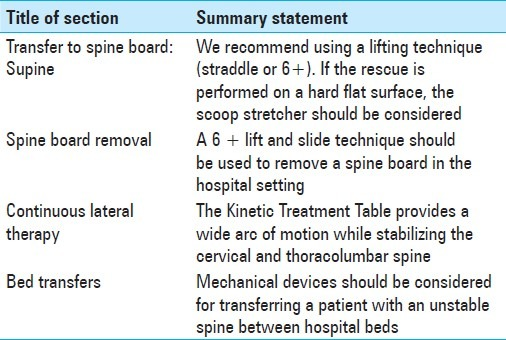
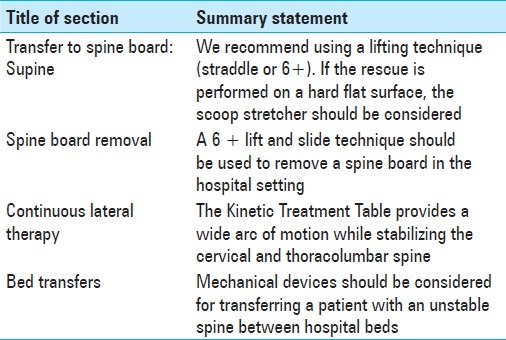
I mentioned that log rolling is becoming verboten, Wuzzie asked about alternatives that are suggested, so I posted the link to the ENA position paper that references alternative methods to move patients instead of log rolling. Is that what you mean? Sorry, brainy no worky today. ?
Thanks for answering. No, I get all of that. I'm just trying to figure out the particulars of exactly what they were trying to clarify with the consensus statement.
I am in the process of finding/reading journal articles that discuss the matter. Thanks! (And thanks @Wuzzie also).
I would always offer on a plane. IMO, the best case scenario is that everyone with medical training will offer and you can discuss amongst yourselves about who is most qualified for this - and who to perhaps confer with if needed. Similar to what was mentioned in the linked article, it can get complicated as to which is the most appropriate/qualified.
an ICU RN, a cardiologist, an NNP, and a radiologist all respond to the emergency call. What is the issue? The cardiologist has had a drink or two, doesn't feel drunk. The ICU RN is a new grad just out of orientation. The NNP is experienced, but that experience is exceptionally narrow. The radiologist is not used to dealing with patients like this - she looks at a computer screen all day.
Chest pains? ICU RN for front line care with the altered cardiologist to give verbal backup and support, as long as they've disclosed their drinking and have stopped (which is why they shouldn't be hands on).
Woman delivering a baby? Radiologist and NNP. The radiologist can take care of the mom, the NNP will take care of the baby. (cardiologist and radiologist both have distant training how to do it, and the radiologist hasn't been drinking).
Seizures? ICU RN with other professionals as backup/extra hands.
Coding? Everyone except the cardiologist can help - but the ICU RN and NNP have more code experience than the radiologist (NNP's codes might be with babies, but you are in a good habit of being in that situation, less likelihood of panic/freezing)
I am not worried about being sued or getting into trouble for offering help. No jury will convict assistance offered in good faith even if someone did sue.
In a situation when I am the only person available and I may have had a drink? If I am literally the only person that can help, I will offer and tell everyone, patient, family, staff, that I have had a drink and I cannot accurately guarantee my level of impairment, but if I'm the only thing you got, I might be better than nothing. In the latter situation, my preferred situation would be to be able to give my observations to another provider who is on a phone (again, disclosing I've had a drink). There are even situations where someone could be totally sloshed and if there is no one else to help, they might still be better than inaction. (for example, if a woman delivered a mildly premature baby, the NNP could make sure they know to do kangaroo care until they can land. That she would know in her sleep. Obviously that would be incredibly terrible as a situation, but the chances of it happening are so extremely rare.
The flight attendants wouldn't automatically know who is most suited, and often if most people won't say they can help, there's no chance to know who could best help.
I do transport as an NNP and even if I was the only person available on a flight, I could at least talk to ground support to give accurate assessments and carry out recommendations. I know there is always ground support somewhere.
I also think back to the case where the woman died on a flight back from Hawaii when they didn't divert when recommended by the doc who responded. That doc made a mistake, IMO, because the first time she lost consciousness (which was written off as syncope due to anxiety, without ever having a history of syncope), the flight should have landed ASAP. It was over an hour later when she had the loss of consciousness with loss of bowel control/seizure. But no one is getting upset at him (likely helped by the fact they were over water with nowhere to land anyway). Even with the mistake, it was given in good faith, and there weren't other people giving other options or disagreeing.
Lots of rambling to say, legal consequences be damned, the moral and ethical thing to do IMO is to offer aid.
I think I'd take the ICU RN over the radiologist to help with mom, but, hey, if we're ever on the same plane together, let's do this.
One of my most vivid childhood memories is of my mother doing an emergent c-section with a framing saw and a butcher knife when one of our cows died during calf-birth. She directed my dad and I to help. We got the calf out too late to save him, but the courageous effort ignited my passion to heal. For better or worse, I have a strong genetic disposition to go for it and deal with a jury later if necessary.
I think I'd take the ICU RN over the radiologist to help with mom, but, hey, if we're ever on the same plane together, let's do this.
One of my most vivid childhood memories is of my mother doing an emergent c-section with a framing saw and a butcher knife when one of our cows died during calf-birth. She directed my dad and I to help. We got the calf out too late to save him, but the courageous effort ignited my passion to heal. For better or worse, I have a strong genetic disposition to go for it and deal with a jury later if necessary.
I choose that because most ICU RNs have had little to no experience with women's health I would think.
Most of the 'do not intervene' crowd seem to fear lawsuits, and the 'assess first before making decision to intervene' crowd seems to have a more logical process to make that choice or not. I believe we as medical providers have a duty to respond to a medical incident if it were to happen pre-hospital to at least see if we can do something. We are all BLS certified to a minimum so I think we should require some sort of aid to be rendered. If someone were to have a broken arm, or something else non-critical then all we could do is provide support both physically and mentally before they go to the hospital themselves or EMS arrives depending on severity. If your own family were to have an emergency occur and you learned a medical professional just walked by you would justifiably be upset that they didn't at least stop and assess the situation. That is why I think at a bare minimum stopping to assess should be required by our duty as health professionals, but the aid rendered is up to the situation but good Samaritan laws most certainly apply. I think I remember getting some of those questions on some tests in RN school and 1 on my NCLEX actually so this is an issue that does get some attention in schools now.
That is why I think at a bare minimum stopping to assess should be required by our duty as health professionals, but the aid rendered is up to the situation but good Samaritan laws most certainly apply.
Respectfully, I don't think this is entirely accurate. There's been situations reported where lawsuits occured because the attending off duty nurse did something that's later proven to be something they were not "specifically trained to do" at the incident scene. The court held them legally accountable and the rest of the story involved the transfer of lots of money in the usual manner.
I'm not discouraging anyone from attending an incident to offer help, but be aware good Samaritan laws don't necessarily protect and stop lawsuits from occurring in every situation. You know, people are always happy to see a nurse stop and help, but the same people sue when the person they are helping dies. Guess, that's how people show their gratitude for some apparent reason. ...I dunno. So probably best to forget about the pen knife and bic pens, and just do the minimum necessary until EMS arrives. They usually show up pretty quickly anyways.
I believe if many of the 'do not intervene' crowd would be singing a different tune if it were themselves or their loved ones who were the ones having an emergency. If I were choking on food an required basic first aid (Heimlich) and an RN was just sitting there watching me because they feared lawsuits afterwards I believe that should be a crime. The same goes for if your spouse were lying on a sidewalk bleeding out and required direct pressure but an on looking MD did nothing because they could imagine their malpractice insurance premiums increasing so they sat and watched this person die. That is why at a bare minimum assessment should be provided to someone who requires aid. Should you do a field cric with a pen and knife? No, that is for Hollywood and military operators to do if they had no choice. Should you provide direct pressure for those who have uncontrolled hemorrhage? Absolutely, I believe it is our duty as healthcare providers to do something other than sit and watch because that person is afraid of lawsuits. Have we litigated care for our fellow humans out of our society? It seems to me that many reasons people become nurses; 'I care for others', 'I like healing people', etc., were nothing but spouted platitudes given the number of 'do not intervene' crowd and their reasoning. Their real reasons seem to be; 'I like the paycheck', 'I like helping people sometimes if I'm paid', 'my duty to heal ends at my shift', etc.
If I were choking on food an required basic first aid (Heimlich) and an RN was just sitting there watching me because they feared lawsuits afterwards I believe that should be a crime.
Quite frankly, I don't see why any RN witnessing such an occurrence would avoid reacting to this situation due to fear of a lawsuit. The risk of lawsuit is virtually non existent and it's pretty cut and dry in this situation.
However, that's not exactly the same situation as one would encounter when a vehicle becomes a part of a tree, with a trapped occupant in distress hanging upside down by a seatbelt inside.
You see, that's the kind of situational event when nurses fear lawsuits.
Respectfully, the line involving fear of lawsuits are not written across the entire spectrum of every situation encountered, and I think it's important to clarify the distinction.
Quite frankly, I don't see why any RN witnessing such an occurrence would avoid reacting to this situation due to fear of a lawsuit. The risk of lawsuit is virtually non existent and it's pretty cut and dry in this situation.
However, that's not exactly the same situation as one would encounter when a vehicle becomes a part of a tree, with a trapped occupant in distress hanging upside down by a seatbelt inside.
You see, that's the kind of situational event when nurses fear lawsuits.
Respectfully, the line involving fear of lawsuits are not written across the entire spectrum of every situation encountered, and I think it's important to clarify the distinction.
That is exactly my point. There are different situations requiring different things and as healthcare providers we cannot know what the situation is until we assess it. If in your example the patient is inside the car wrapped around the tree, well not much besides emotional support we can do most likely. Other situations may be more direct as I mentioned, regardless an assessment should be performed to see if help can or cannot be given based upon situation.
I mentioned that log rolling is becoming verboten, Wuzzie asked about alternatives that are suggested, so I posted the link to the ENA position paper that references alternative methods to move patients instead of log rolling. Is that what you mean? Sorry, brainy no worky today. ?
Thanks for answering. No, I get all of that. I'm just trying to figure out the particulars of exactly what they were trying to clarify with the consensus statement.
I am in the process of finding/reading journal articles that discuss the matter. Thanks! (And thanks @Wuzzie also).

Wuzzie
5,243 Posts
I think that this is what has changed and may not be clear. It seems that what they have found is injury to the spine below C1-7 is statistically unlikely in most head injury scenarios and that the current treatment (backboard+c-spine immobilization) does not meet risk-benefit standards. However, any impact hard enough to cause head injury symptoms has a higher probability of having associated cervical vertebral issues mostly due to the extreme mobility of the neck vs say the lumbar spine. I disagree that you cannot immobilize the cervical spine without immobilizing the remainder. Certainly placing a c-collar and then letting the patient walk around is useless but a c-collar and hands on or putting the patient supine on a firm (not hard) surface is adequate.