I've come across patients, usually post op, that needs to be routinely assessed on their pain levels.
Now I'm trying to look for a way to ask them on their pain level without planting into their minds the idea that they're actually feeling pain. Of course we can plan a response from their report, but we might be addressing pain that is actually not present in that moment.
Can we ask a general question of "how are you feeling right now?", instead of "are you feeling any pain right now?" Should we be direct or indirect in these kind of situations?
Pain is what the pt. says it is. You have no other way of determining that than by asking. Yes, there are physical signs of pain, as well as physical signs of NOT being in pain, but that's subjective and the only way to find out is to ask.
Your job is not "Pain Med Police." Your job is to relieve perceived pain, whether you believe it really exists or not.
I always ask "on a scale of zero to ten zero being no pain and ten being the worst pain of your life, how much pain are you in right now?" Per my facility's policy, I must have a number. Now if they say ten and then I observe them laughing with friends and playing on their phone...I chart what I see. But I don't try to skirt around asking about pain to avoid "planting ideas" in their mind.[/quote']
Can I just say to this I have given pain scores of 9-10 and done exactly that....it all depends on the level of tolerance....they soon discovered I had a gangrenous appendix which fell apart as it was being removed but my pain threshold is extremely high! So just because someone is laughing or on their phone doesn't mean they are not in pain.
I had a doctor last year tell me I couldn't have a pain score of 7-8 because I looked perfectly well...it got back to him after I had a lumbar puncture that my opening pressure was 44! Never make assumptions unless you can be 500% sure you're right!
How is your pain? Even If they deny pain, I usually make them rate it and I don't go further if it is a 0. 1-3: ill see if repositioning or mild pain relievers help. Moderate to severe is going to get heavier duty pain meds.
I try not to snow anyone but I will not be a gate keeper and try to weasel out the fakers. It's not my place to call anyone out on lying and if they are living and breathing okay, they are okay with me. I enjoy work SO much more now with this outlook.
Specializes in PICU, NICU, L&D, Public Health, Hospice.
I find that hospitalized people(patients) often respond better to the "pain" questions and the 1-10 scale than do patients in their homes, and the very elderly.
Too often elderly people don't count their aches as pain.
Our language can affect how people answer us, especially if there are cultural issues at play. An Athabaskan indian may answer about pain quite differently than say an Irishman.
In my view, as nurses, it is our obligation to have a GOOD appreciation for the comfort needs of the patients under our care. For some that can be determined easily and quickly, for others we must dig a bit.
Specializes in Med-Surg/Neuro/Oncology floor nursing..
Sorry to go off topic for a second but this reminds me of an episode of Nurse Jackie I was watching last night...they asked a patient(played by John Cullum) what his pain was on a scale from 1-10(he had end stage liver cancer) and his response was.."it only goes up to ten?" Boy have I been there.
Anyway on neuro we deal with a lot of neurosurgeries/TBI's so I am constantly checking on my patients pain. I like to be as direct as possible and find the number scale works the best. My patients have had their skulls opened up/positive ct scans/mri's so I know they must be hurting and drug seekers really aren't an issue(of course they could exaggerate to get high doses of meds...but I am not the DEA). I also look to see if/when my patients last dose of medication was and I will ask them if it helped, made them feel better and if they feel like they need more. I myself had a crani for trigeminal neuraglia and there was a complication and a 2 hour surgery turned into 5 hours so the pain was intense. I was also a chronic pain patient BEFORE the surgery(still am) so my baseline was higher to begin with...and I had no problem being vocal about my pain. When dealing with chronic pain patients with acute issues and they say they are an eight I ask what is hurting them...their surgery site or their herniated back disc.
When I work on oncology(once in a while when I am needed) I am extremely aggressive about my patients pain. I definitely check in on them often. Most of the time they have PCA's and are visited by pain management daily...but still cancer pain is something I do not want to mess with(I don't want mess with any pain actually).
As for the are you comfortable question...I try to avoid it because being flat on your back in those beds alone can make you uncomfortable.
I've come across patients, usually post op, that needs to be routinely assessed on their pain levels.
Now I'm trying to look for a way to ask them on their pain level without planting into their minds the idea that they're actually feeling pain. Of course we can plan a response from their report, but we might be addressing pain that is actually not present in that moment.
Can we ask a general question of "how are you feeling right now?", instead of "are you feeling any pain right now?" Should we be direct or indirect in these kind of situations?
Is that possible? Thanks for your time! :)
Why would you assume that if patients answer affirmatively to the question "do you have pain?" that it's because you planted the idea of pain in their heads? Having surgery hurts and post-op patients should be assessed for pain regularly and medicated.
When I worked in the hospital (pedi neurology/neurosurgery), I flat out asked the older kids "does your head (or your back for spinal surgery kids) hurt?" If they said yes, I asked them how much by using either the Wong-Baker FACES scale or the standard 0-10 scale. Then I asked them (or their parents) "do you want/need to take medicine for it?"
Specializes in Acute Care Cardiac, Education, Prof Practice.
In the hospital is the last place I would want someone to be unclear with me. If I want to know if my patient is having pain, then I ask them if they are having pain and then use the appropriate pain scale to determine what the appropriate nursing intervention is. It is not my place to try and deter a subjective measurement by attempting to skirt around the subject of pain, and I definitely do not want my patient to be undertreated for pain.
Specializes in Med Surg, Homecare, Hospice, Rehab.
A tactic I have used if I see no visible signs of significant pain/discomfort (including my somatic/gut response regarding their position in bed or chair:
I have asked "How are you feeling?" and after their reply, if meds not quickly indicated, often asked, "How are you feeling about how you are feeling?". I have often saved that for post Rx assessment as well.
In truth, I have received some "interesting" answers (!).
And how we go about it may be as important as the response(s) we receive . . . I have not seen any nurses this insensitive, yet:
- I had been Rx'd some Physical Therapy to assess for efficacy of therapy vs manipulation under anesthesia.
The Therapist was assessing for range of motion, said he, and proceeded to move my (L) biceps to my toward my left ear and saying, "Tell me if this hurts on a scale of 1-10. He pushed hard.
I had sparks in my eyes. I could not breathe and he was lifting my hips against the resistance (along with my trying to decrease the searing pain caused by his "assessment") and managed to barely squeak out "50!".
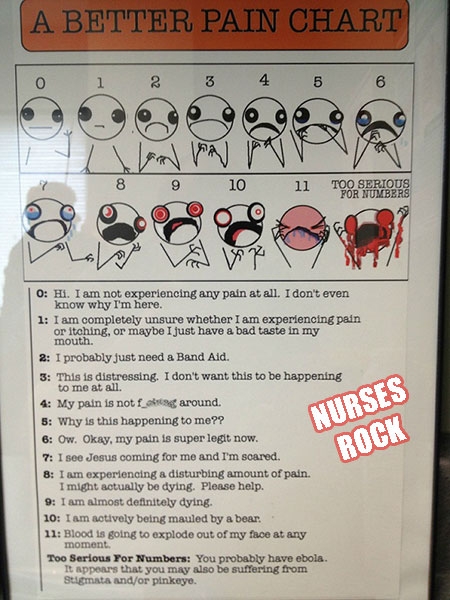
. . . Please see the face past "11" above and instead of tears, draw in RAGE ! . . . (I love that chart - as well as the Samurai Maxim.)
He relaxed his push a bit and said, "You can't have fifty."
My response, as I gasped for breath was, "THE HELL I CAN'T! ! " and wrenched my (L) arm from his grasp with my right.
(I swear, I had been able to breath I would have tried to rip his head off . . .) and yes, he stepped back quickly, and he only being half-again bigger than my size. (Not once did that %#%$ say he was sorry).
Just for the record - when having the manipulation a week or so later, my Orthopod said there had been a lot of popping and snapping and my whole upper arm was a mass of purple bruises - I asked him if my shoulder had been "Epoxied" He said, "Close".
After the manipulation took 3 months of therapy (at another place) to get my range restored - in which I learned of Iontophoresis vs PO meds.
I guess I have taken the long way of saying there is really only one best way to assess a patient's pain: the trial-and-error approach to learning what works best for each patient.
I learned well in years past . . . "Puppy love is real to the Puppy" (see Maya Angelou) and have opted for a more eclectic approach.
One CPE Supervisor often counseled,"Do or say the obvious".
EDIT:
All that said, I have often offered male patients the suggestion that they not "wait until they cannot wait" until asking for pain Rx. I tell them that, in my experience (with Hospice too) it often takes more Rx to get it under control than if they deal with it sooner. I have countered the, " ... but I am afraid of getting adicted ..." with: "Our goal is to adjust the meds to the symptoms. As the symptoms diminish as you heal, the meds are reduced as well. We will work this together".


NurseDirtyBird
425 Posts
Pain is what the pt. says it is. You have no other way of determining that than by asking. Yes, there are physical signs of pain, as well as physical signs of NOT being in pain, but that's subjective and the only way to find out is to ask.
Your job is not "Pain Med Police." Your job is to relieve perceived pain, whether you believe it really exists or not.