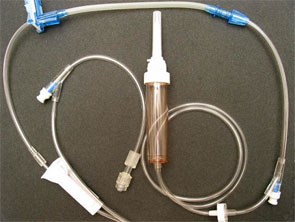
The hospitals in this city use the Alaris pump and this kind of Alaris infusion set:
Prior to my preceptorship, I've always twist that end cap a little bit so that the IV solution can dribble out while priming.
However, during my first shift of my preceptorship, my preceptor didn't agree with my method. She said just to let the IV solution flow to just before the end of the line, put in a threaded cannula and then let the solution dribble out. She mentioned that my method would cause the end to be non-sterile?????
Can someone shed some light on this as my previous clinical instructors have seen me prime IV lines and they never had a hissy fit about the way I do it.