I am truly interested in having a positive discussion that attempts to answer the questions I posed here. But I am also reacting to the long discussions among at least three threads regarding the nurse charged with homicide. I don't believe a perfect human exists.
Let's define "perfect nurse" so we can know how to be one. A perfect nurse is one who never makes a mistake. One who never makes a medication administration error and therefore adheres to all patient rights of medication administration every single time without fail. One who adheres to all professional standards of practice throughout every second of every work day. One who distinguishes between being a "good worker" and a "good nurse" and so knows when to stand up to her boss and refuse work assignments. One who knows her limitations, so can anticipate coming across something she might not have learned yet and will avoid being put into situations that might cause her to exceed her limitations. One who will always without fail ask for help when needed and ask or look something up before doing something new.
The nature of nurses' work and their role as "last line of defense" in patient safety demands that a nurse be able to think critically. So the nurse's brain is the utmost important tool in her work belt and must remain sharp. Brains are complex and often fail unexpectedly in people of all intelligence levels...e.g. looking for glasses when they're on your head. Brains can have moments of lapses when people are: fatigued; sick; distracted; overloaded with information; under intense stress; etc. Yet a perfect nurse does not have brain failure...EVER. A perfect nurse can work 12 hour shifts and still not have one single second of brain failure...EVER.
Questions for Consideration:
1. Is it possible to be a perfect nurse in an understaffed hospital? Is it possible to be a perfect nurse in any imperfect work environment? (Yes? -Tips to do so?)
2. Tragically, being a "good worker" is too often in conflict with being a "good nurse". If a working nurse is striving hard to please the boss due to her high work ethic, she quite possibly is failing to ensure patients' safety by taking on more than she can handle. So how do we reconcile nursing school knowledge and professional standards of practice with current unsafe conditions of many nursing jobs? Do employers have any obligation to make being a "good worker" the same thing as being a "good nurse" -- or does it all fall on the nurse to be perfect when faced with imperfect demands in an imperfect environment?
3. How can work environments, administration of health facilities, nursing schools, health care laws, or other entities which affect nursing jobs make it possible for the perfect nurse to remain perfect at all times in her job?
4. If any of you nurses have never experienced a second of brain failure (especially not a full 30 min. or more of brain failure), and if any of you are incapable of skipping one or more med. admin. safety steps despite any environmental circumstances, and if any of you declare yourself to be a perfect nurse as defined here...do you have tips to help the rest of us become more like you? This is a serious question and I for one am grateful you are a nurse, grateful for your service, and would be grateful to learn from you. Because truly, what nurse wouldn't want to be perfect? Sign me up!
Disclaimer: I don't believe there exists a perfect nurse who is incapable, regardless of any imaginable circumstances and environments, of skipping multiple safety checks in medication administration. Yet some claim to not ever be capable of such grave errors. To ignore the potential of our brains to fail and to so willingly condemn the charged nurse as a criminal without even knowing what was going through her mind and what circumstances and environment led up to her giving the wrong medicine is scary to me and lacks something the perfect nurse would surely have: compassion; the desire to understand; the desire to remedy rather than penalize; the desire to heal.
Some will say she should no longer be a nurse because she failed too badly in the professional standards of practice. I believe she was being mindless so never made the choice to skip any safety measures; I believe she had every intention of helping patients and that she took it for granted that she had no chance of harming them because she believed in those moments that there was no chance. I believe it was an accident that would not have happened in ideal work conditions, and I can imagine many things leading to a nurse becoming mindless through no fault of the nurse. Maybe she should never be a nurse again or maybe she would be the best nurse in the world after this experience. I'm not forming an opinion on non-criminal consequences right now. I try in the "Nurse Charged with Homicide" thread to convince you why, from what we know so far, the case does not warrant criminal charges. What should have been in her mind and what was ;in her mind are two different things, and that difference is why she is not a criminal for being in a mindless rush to give a medicine she believed would not harm the patient and then to not monitor the patient because she believed the patient was unharmed by the medicine. That's just my interpretation of the law. Don't forget, law is subjective so you get to have your interpretation too; I just hope judge and jury have more in common with my way of thinking. I hope this nurse doesn't spend a day behind bars when she likely was just trying to be a "good worker" and not experienced enough to focus solely instead on just being a "good nurse"
Anyhow, though writing this was inspired by my strong feelings in the other threads, we could keep our continual conversation about this case in the other threads (if you want) and save this particular thread for positive, creative ideas that might answer some of the questions above.
Also, there is a well-written and worth-reading article in this forum Is It Possible to Never Make an Error? The Perfect Nurse Fallacy by @SafetyNurse1968 (I wrote this and forgot that article was already broaching these topics!), but the discussion following it didn't seem to have a lot of tips from any perfect nurses for how to be perfect in understaffed hospitals or otherwise unsafe work conditions, so I'm trying here too.
What you are describing is called "Situational Truth".
"In that moment, I believed this particular thing to be true."
That's not how I want my nurse to behave. Nor anyone that would lay a single finger on someone I love and care about.
Situational truth is for cheaters and liars. "Well....I believed at that moment, that you didn't love me anymore, so it was okay to pick up that hooker."
See how that goes? I can say....whatever will get me out of the hot seat..."at the time" I believed such and such. There's no proof whatsoever what was in her mind at the time---only ACTIONS count.
Which, if I am correct in assuming---is PRECISELY what CMS, the prosecutor and the TBON is about to judge her over.
The road to hell is paved with good intentions, MtnRN. And RV may have a heart of gold, but so does a hard boiled egg. She needs to find another line of work---and the TBON needs to make sure that she never, ever practices nursing again---particularly since she cruised off to her job at Centennial without a g*****n word to anybody about her past.
Specializes in CCU, SICU, CVSICU, Precepting & Teaching.
On 2/11/2019 at 4:22 AM, HomeBound said:
I like MtnRN. She's quite passionate in something she believes to be true. However, there just doesn't seem to be a middle ground with her. It's one extreme or the other...case in point. If you follow the rules and are trying to hold someone accountable for their rule breaking, you believe you are "perfect" and the implication is, that some of us feel that since we've gone >10 years with no med errors...we believe we're better in some way.
It wasn't the point, MtnRN, and this diatribe really does speak to how the extremes never help a situation. I was middle of the road. I fell on the side of unemotional, factual and lawful critique of Ms. Vaught's individual situation...as all crimes should be considered on a case by case basis.
I did read your manifesto. I think that having a clean as a whistle record (mine) for as many moons as I've been in the profession...as well as those others who have done the same...by following the rules...YES...every. single. time. (are you advocating for following rules only sometimes...because it makes you an orificehole because you're just so uptight about those rule thingies?)....is something to do a little chest thump about---because it's stressful, time consuming, and takes aaaaaaaaaaaaall the damn fun out of using work as a social tool.
I cannot believe that there is anyone who has "worked many moons" who has not made a mistake. Who follows the rules EVERY SINGLE TIME and never gets distracted, or puts down a vial to open a syringe and then picks up the vial right next to it, who notices every single time the pharmacy puts the nitride in the nitroglycerine slot or an order is written incorrectly or a patient, who has willfully removed their wristband and cannot remember their own name or birthdate is on the wrong side of the room. I cannot believe there is any one of us who is absolutely perfect.
I try very hard, I follow the rules every single time -- until there's a situation that falls outside the rules, that the policies haven't accounted for and we have to make things up as we go along. Sometimes, the rules don't keep up with changes in medicine. Sometimes, I have a brain fart. I have made mistakes.
The difference between me and you is that I KNOW I have made mistakes and I know I'm capable of making more mistakes in the future. I will recognize my mistakes because I am allowing for the possibility and double-checking yet again. You don't know how many mistakes you've made and won't be willing to consider the possibility that you might make one or HAVE made one. So you won't recognize your mistakes, won't set about to mitigate the harm to the patient.
I'd much rather be cared for by the nurse who has made mistakes and learned from them. Really.
I have made mistakes. Admitted to several in this thread with the negligent nurse. Titrating insulin drip down instead of leaving it alone. Reported myself. Pulled 2 of x drug instead of 1 or vice versa.
I'm talking about medication errors that you went right ahead, gave a medication, did a treatment (like lopping off the wrong limb or doing the chest xray when it wasn't ordered or needed), or otherwise plodded right along and did your thing---maybe noticing, maybe not.
I supposed you just had to chime in with it, because you haven't actually read where I admit many, many times that I make mistakes....and somebody just has to defend a poster that really just wants to believe that RV was in dreamland and just could never, ever be held responsible for her actions, because....brain fart for a whole day. (which is what RV's behavior would have to amount to)
I have been in medicine for 26 years, sweetheart. Graduated in 1993. So the snark can be filed exactly where it should go. Ruby, I like most of your posts, and I understand where you've been, because guess what---you don't have the corner on the market for what's happened to you. Some of us simply keep it to ourselves a little more. Demeaning and condescending to nurses that YES----FOLLOW.THE.RULES.EVERY SINGLE TIME---is just projection that because YOU may not follow them, nobody else could possibly do so.
I misread a chart on insulin. I didn't NOT LOOK AT IT and just "wing it". I didn't ask for help when I was confused about wording. RV just blew through everything, because she was just so important there, with her preceptee and all....yapping about the all important "can you swallow an ice chip? Good. Now, can you swallow 1 tsp of water? Good. Now, can you say EEEEEEEE?" Sorry. I don't defend people who can't get their head in the game when they see an order for a benzo or a narcotic or a vasoactive and there aren't big red alarm bells dinging all over the place to PAY ATTENTION TO WHAT YOU ARE DOING.
I made a mistake ambulating a GI Bleed patient, against my better judgement, because I let that orifice bully me. He went down, and I went down with him, with a crushed SI joint for my trouble.
So don't. Don't even think you know how I work, how long I've worked or what my experiences are. I have had to self report 3 times---and that is enough for me to make gd sure I slow my roll. I also have a family member that ended up on the floor because of nurses like RV and others with "brain farts" all day long---after her AAA surgery....because someone just couldn't get off their super experienced orifice and get her a bedpan. So don't assume you know anything about me or my work ethic.
Specializes in CCU, SICU, CVSICU, Precepting & Teaching.
38 minutes ago, HomeBound said:
RV
I have made mistakes. Admitted to several in this thread with the negligent nurse. Titrating insulin drip down instead of leaving it alone. Reported myself. Pulled 2 of x drug instead of 1 or vice versa.
I'm talking about medication errors that you went right ahead, gave a medication, did a treatment (like lopping off the wrong limb or doing the chest xray when it wasn't ordered or needed), or otherwise plodded right along and did your thing---maybe noticing, maybe not.
I supposed you just had to chime in with it, because you haven't actually read where I admit many, many times that I make mistakes....and somebody just has to defend a poster that really just wants to believe that RV was in dreamland and just could never, ever be held responsible for her actions, because....brain fart for a whole day. (which is what RV's behavior would have to amount to)
I have been in medicine for 26 years, sweetheart. Graduated in 1993. So the snark can be filed exactly where it should go. Ruby, I like most of your posts, and I understand where you've been, because guess what---you don't have the corner on the market for what's happened to you. Some of us simply keep it to ourselves a little more. Demeaning and condescending to nurses that YES----FOLLOW.THE.RULES.EVERY SINGLE TIME---is just projection that because YOU may not follow them, nobody else could possibly do so.
I misread a chart on insulin. I didn't NOT LOOK AT IT and just "wing it". I didn't ask for help when I was confused about wording. RV just blew through everything, because she was just so important there, with her preceptee and all....yapping about the all important "can you swallow an ice chip? Good. Now, can you swallow 1 tsp of water? Good. Now, can you say EEEEEEEE?" Sorry. I don't defend people who can't get their head in the game when they see an order for a benzo or a narcotic or a vasoactive and there aren't big red alarm bells dinging all over the place to PAY ATTENTION TO WHAT YOU ARE DOING.
I made a mistake ambulating a GI Bleed patient, against my better judgement, because I let that orifice bully me. He went down, and I went down with him, with a crushed SI joint for my trouble.
So don't. Don't even think you know how I work, how long I've worked or what my experiences are. I have had to self report 3 times---and that is enough for me to make gd sure I slow my roll. I also have a family member that ended up on the floor because of nurses like RV and others with "brain farts" all day long---after her AAA surgery....because someone just couldn't get off their super experienced orifice and get her a bedpan. So don't assume you know anything about me or my work ethic.
I don't you, don't know your practice, and have not made a practice of following new posters with relatively few posts. I'm not judging your work ethic, your practices, or anything except the post that I quoted.
Quote
I think that having a clean as a whistle record (mine) for as many moons as I've been in the profession...as well as those others who have done the same...by following the rules...YES...every. single. time. (are you advocating for following rules only sometimes...because it makes you an orificehole because you're just so uptight about those rule thingies?)....is something to do a little chest thump about---because it's stressful, time consuming, and takes aaaaaaaaaaaaall the damn fun out of using work as a social tool.
I don't believe that anyone can have a perfect record of no medication errors as you brag of having in the quoted paragraph. That was my point. If you honestly believe that you never have and will never make a mistake, then you're dangerous because you won't recognize when you've made one.
Your response to me indicates that you have made mistakes, you've been aware of it, and that I should know that, too. But I don't know you. So forgive me that I've missed the posts where you admitted to your errors and only saw the one where you boasted of having a "clean as a whistle" record.
Because from where I'm standing, a "clean as a whistle" record could only come from never noticing your own errors or actively covering them up.
I don't you, don't know your practice, and have not made a practice of following new posters with relatively few posts. I'm not judging your work ethic, your practices, or anything except the post that I quoted.
I don't believe that anyone can have a perfect record of no medication errors as you brag of having in the quoted paragraph. That was my point. If you honestly believe that you never have and will never make a mistake, then you're dangerous because you won't recognize when you've made one.
Your response to me indicates that you have made mistakes, you've been aware of it, and that I should know that, too. But I don't know you. So forgive me that I've missed the posts where you admitted to your errors and only saw the one where you boasted of having a "clean as a whistle" record.
Because from where I'm standing, a "clean as a whistle" record could only come from never noticing your own errors or actively covering them up.
Thank you. Perhaps I did mislead after re-reading my post. My intent was that I have no serious problems in my practice---my record is clean. I have never, ever been charged, written up, talked to or otherwise pulled up hard over any type of thing that I've done.
I did, once, mislabel a blood draw tube--a pink top for transfusion--and put the wrong patient's label on it---because I skirted the rules of the triple check. I had it in my hand and I "knew" it was right---and didn't re-read the label. The lab caught it like---pronto---called over and I reported myself to my manager. She wasn't phased, but said, "Don't do it again." I never did it again.
Like putting your hand on a hot stove. You only have to do that once and the fear is permanent, at least, in some people.
Which is my point. RV had the fear put in her. In nursing school. In seeing ICU patients and critical care. In taking all of the exams she did in order to be where she was. She cannot have faked all of that. She had that knowledge in her mind, and she either does not understand the repercussions of her actions, or she does not care.
Either way, she should never have been in her position because of it---and now a woman died a horrifying death because of RV's negligent, and yes, I will say it, abusive behavior.
Because, Ruby, as you and I may intimately know---it's abuse to violate the rights of another human being.
Perfection does not exist. As far as mistakes being made, it depends on the work being completed. Everything changes so it not possible to know everything.
Nobody expects nurses to be perfect, but what you are expected to do is follow policies.
They are written for a reason.
In every unit there is always this small group of nurses with the "I'm not going to be bothered" attitude that cause problems for everyone else that is following policy. So when one of their sloppy moves causes a problem with a patient, there is a huge investigation, everyone has to come in on their days off for inservice, new policies so it doesn't happen again, blah, blah, blah. So everyone on the floor gets punished because ONE PERSON didn't follow the rules.
I fully support professional Darwinism: Get rid of the problem nurses.
Yes! That exactly. Every time a new "staff education" comes out you know that somebody screwed up. Then comes the new policy for whatever the screw up was that invariably adds to the already way too much busy work we have. What ever happened to educating and if necessary disciplining the nurse who performed the error?
Plus the current model only draws attention to the fact that somebody committed an error of some kind that is resulting in additional work for all nurses. Not exactly good for morale.
What I've gathered from comments so far is that nurses cannot be perfect (in fact no one can be), but that we should strive to at all times to follow policies and standards of practice and be willing to quit or be fired when we refuse to put ourselves in situations that compromise patients' safety. People have pointed out we should also admit and report when we do make a mistake and learn from it. That is all very good advice. There's also plenty nurses should do to ensure their most important tool at their job (brain) is ready for the work day, e.g. plenty of sleep the night before.
Any ideas about the role of facilities in keeping nurses' most important tool sharp enough to get the job done safely? How much is the employer's responsibility? For example, brains are more likely to fail when a nurse works 12 straight hours without adequate breaks. Doubling up on patients is not a good idea when safety is the highest priority. What are some methods of ensuring every nurse gets an uninterrupted lunch break?
A tip related to my first question, which I've found in this forum recently:
Be good and ready to quit or be fired if bosses demand you take an unsafe assignment (how to always know what might unexpectedly become unsafe without enough experience, I'm not sure). This is difficult to do when you rely on a job. It's also difficult to do when you've had a high work ethic your whole life and then find yourself in a profession where you absolutely must say no to your boss even while they nearly convince you that you can handle it. More tips related to this -- in fact, a whole class in nursing school devoted to this very topic -- would be helpful in keeping patients safer.
This is something useful that's new to me (copied from homicide thread):
Quote
23 hours ago, juan de la cruz said:
nurses can fill out an "Assignment Despite Objection" form as a way to tell the manager that "yes, I'm not going to abandon my patients but you're putting me in an unsafe situation and you can be held liable if something were to happen".
* Pass laws requiring health facilities to make "good worker" compatible with "good nurse", e.g. where cutting corners isn't required to satisfy demands of the job. This can partly be accomplished with mandatory maximum patient loads. Other ideas for how to force facilities to have reasonable, safe work expectations of nurses (and CNAs, doctors...)? Oh yeah, perhaps form a union!
* Reduce constant warnings and alerts that are redundant or not absolutely necessary. This person said it best in another thread:
Quote
On 2/14/2019 at 9:33 AM, Emergent said:
I think that's a big problem, that we are getting bombarded with constant warnings and alerts, many of which are redundant. We end up tuning them out because that's what the human brain does.
* Daily reminders during shift change announcements to slow down, put safety first always, and call for help. And back that up by having enough staff to allow for help when needed.
* Put med scanning capability in radiology
* No doubling up on patients, even to cover for lunch breaks. Have sufficient uninterrupted lunch breaks that does not require other nurses to double-up on patients.
* 12 hour shifts...a good idea if safety is the highest priority, considering how sharp a nurse's brain must remain the entire shift??
What I see as the top priority solution regarding my third question is this:
Mandated maximum number of patients! -- for Nurses, CNAs, Doctors, NPs, PAs, ALL HEALTH CARE PROVIDERS!
I don't know how much this has been discussed on this forum, but as big a deal as it seems to me, I'm surprised by looking at allnurses homepage, then at the 'What's Happening' side column, and at the 'What's New' top tab, there is no screaming message on this topic...no message at all on this extremely important and urgent topic. Isn't this a HUGE DEADLY problem all over the country right now? Why isn't someone screaming about it every single day? Everyone might have been and just taking a break for all I know. So anyhow, I'm going to scream about it here. We cannot scream about this too much! If I had the money, I would fill the message on billboards all around the country!
What is the point in ANY safety protocol or warning signs or beeping alerts, etc. if there is not enough staff to attend to patients and keep them safe?!?! Patients will not be safe if there is not enough staff!!! You wonder why a doctor's urgent order was overlooked? Why a pressure ulcer developed? Why a total-care patient went hungry for dinner? Why patients fall out of bed attempting to get to the bathroom because their call light wasn't answered? Why sepsis wasn't identified soon enough to prevent death? Why medication administration errors are made? Why a life-threatening arrhythmia wasn't noticed on the telemetry monitor? Why patients are angry because nobody is telling them what's going on and they don't even know who their nurse is for the day? Why post-op patients are crying for overdue pain medicine? Why patients lie in feces for hours? Why patients are dying from failure to rescue?
Most nurses became nurses because they want a job where they can help people. MOST of the time, the reason horrible things occur in health care is because there is not enough staff, and most of the time there is not enough staff because money is the bottom line in most health care facilities!
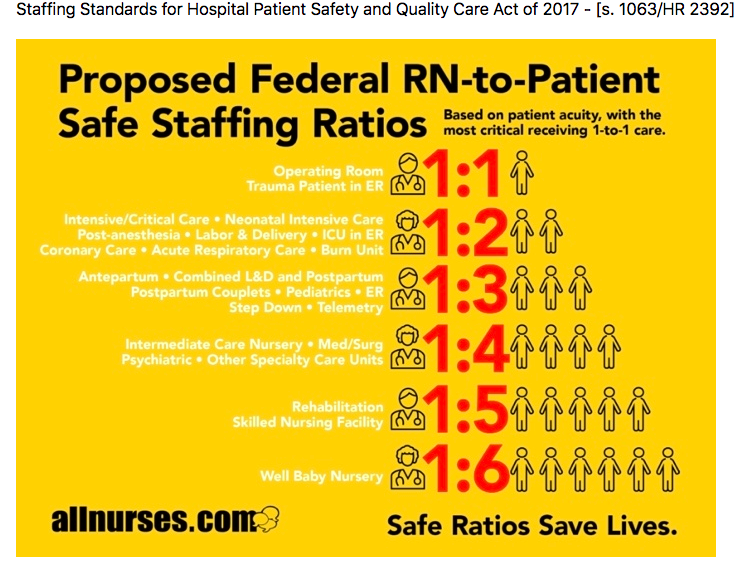
I would go along with the following recommended nurse to patient ratios being safe IF AND ONLY IF there are ALSO enough CNAs for those patients, and those CNAs ALSO have reasonable safe CNA-to-patient ratios and IF AND ONLY IF there is not HIGH acuity for every single patient. If there aren't enough CNAs or if acuity is high for every patient, those ratios would need to come down accordingly.
I am a nurse with only three years of Medical-Surgical experience writing how I feel about safe nurse to patient ratios. If some of you more experienced nurses can safely handle more, fine. But understand that it is NOT SAFE for MANY new grads as well as less experienced nurses to handle more.
Patients will continue to be harmed or die UNTIL WE FIX THIS!!!
Thank you to whoever made this image I am posting here and to whoever is working to pass such legislation!!! (image in next post)
What I suggest could be safe, given my "IF AND ONLY IFs above" is no more than this number of patients:
1-2 patients ICU
3-4 patients MedSurg
4-5 patients SNF
Disclaimer: No, I do not have evidence that understaffing is the reason horrible things occur in health care most of the time. If you have time to do the research and come up with evidence to support or contradict this belief of mine, I welcome your input.

HomeBound
256 Posts
BTW,
What you are describing is called "Situational Truth".
"In that moment, I believed this particular thing to be true."
That's not how I want my nurse to behave. Nor anyone that would lay a single finger on someone I love and care about.
Situational truth is for cheaters and liars. "Well....I believed at that moment, that you didn't love me anymore, so it was okay to pick up that hooker."
See how that goes? I can say....whatever will get me out of the hot seat..."at the time" I believed such and such. There's no proof whatsoever what was in her mind at the time---only ACTIONS count.
Which, if I am correct in assuming---is PRECISELY what CMS, the prosecutor and the TBON is about to judge her over.
The road to hell is paved with good intentions, MtnRN. And RV may have a heart of gold, but so does a hard boiled egg. She needs to find another line of work---and the TBON needs to make sure that she never, ever practices nursing again---particularly since she cruised off to her job at Centennial without a g*****n word to anybody about her past.