A lot of people seemed to like my last real-life case study and I had another interesting one last night... so thought I'd post it.
Here goes...
40-year-old woman was at work when she experienced sudden and acute onset of numbness, tingling, and weakness in her R arm and the R side of her face.
She was rushed through triage to an open room but none of the pod nurses heard the call... I got involved when a call went out that "Dr. Bill needs nursing assistance in room 8." I walked in to see one nurse starting a line on her right arm, someone getting her onto the monitor, someone else getting the EKG set up...
What do you suppose was my first action? What transpired in the first few minutes? What other pieces of information do we need STAT as we talk this through?
Come play the game with me, even if you don't know the answers.
Why the STAT CT? What are we looking for, even before the radiologist sees it?
This lady appears to be having a stroke based on the neurologist's exam. The big question is, ischemic or hemorrhagic... If the former, tPA can save her brain... if the latter, tPA will kill her...
[*]If I could only get one tube of blood, run only one test, which would it be?
Yes!! INR... Bleeding after tPA is always a concern...
[*]Why multiple lines? Why is large-bore (a) unnecessary and (b) even possibly even counterproductive?
Multiple lines: 1 dedicated to the tPA, 1 for drawing labs, 1 for other fluids and meds... 2 lines minimum, 3 is better... and remember, you don't want to be poking somebody after tPA so make sure you've got solid lines.
No large bore is needed because you don't need to fluid resuscitate these people.
The larger the bore, the more likely it is to result in irritation to the vein and the more trauma on insertion... put in the line you need, *not* the biggest one that you can
[*]Why the EKG and fingerstick? (Esme already hit this)
[*]And what about the blood pressure? Is it an issue at this moment? Why or why not? If so, what do we do?
BP is a huge issue because of the risk of bleeding in the brain. At our facility, an SBP>180 is a contraindication to tPA.
The neuro doc ordered labetalol titrated for effect.
[*]What one small, and often incidental, piece of information do we need about this patient? (that nobody has yet touched on)
Weight... tPA is a weight-dosed drug...
So, everything was done, doc and patient decided on tPA... I had an ICU assignment so the patient was delegated to me. We moved the patient to my room while the pharmacist was mixing the tPA.
So, now this is *my* patient, I've an order for tPA and an order for a labetalol drip.
I cycle the bp... down to sbp=162...
Besides the patient identifiers and the order in the MAR, what do I need to check/assess/confirm before I hit this lady with a tPA bolus?
Maintenance of an adequate Cerebral Perfusion Pressure is a cornerstone of modern brain injury therapy.
After brain injury, and especially in the multiply injured patient, cerebral blood flow may be lowered to the ischaemic threshold. To prevent further neuronal death (the secondary brain injury), this flow of well oxygenated blood must be restored. There is no class I evidence for the optimum level of CPP, but 70-80mmHg is probably the critical threshold. Mortality increases approximately 20% for each 10mmHg loss of CPP. In those studies where CPP is maintained above 70mmHg, the reduction in mortality is as much as 35% for those with severe head injury. Cerebral Perfusion Pressure may be maintained by raising the Mean Arterial Pressure or by lowering the Intracranial Pressure. In practice ICP is usually controlled to within normal limits (
^^^this is from the Trauma site you gave the link to...is an increased MAP in either stroke type actually a good thing? Is there an upper limit on CPP (we haven't covered this yet so I am a little confused on it...trying to make sense from the equations and such!!) So as ICP rises, you would also want a rise in MAP to maintain that 70-80 mmHg CPP??
So, everything was done, doc and patient decided on tPA... I had an ICU assignment so the patient was delegated to me. We moved the patient to my room while the pharmacist was mixing the tPA.
So, now this is *my* patient, I've an order for tPA and an order for a labetalol drip.
I cycle the bp... down to sbp=162...
Besides the patient identifiers and the order in the MAR, what do I need to check/assess/confirm before I hit this lady with a tPA bolus?[/QUOTE]
**Second independent check of order and dose calculations??
What one small, and often incidental, piece of information do we need about this patient? (that nobody has yet touched on)
Weight... tPA is a weight-dosed drug...
Aha...I noticed that when I finally looked at my drug guide, but I was pretty stuck on something to do with her being a woman of child-bearing age so I doubt I would have gotten weight!!
Specializes in Critical Care, ED, Cath lab, CTPAC,Trauma.
If the CPP is too low there is poor perfusion to the brain because the B/P is too low to get the blood to the injured brain due to swelling. If it is too high, usually >90-110 there is poor perfusion to the brain as there is too much swelling restricting blood flow to the brain.
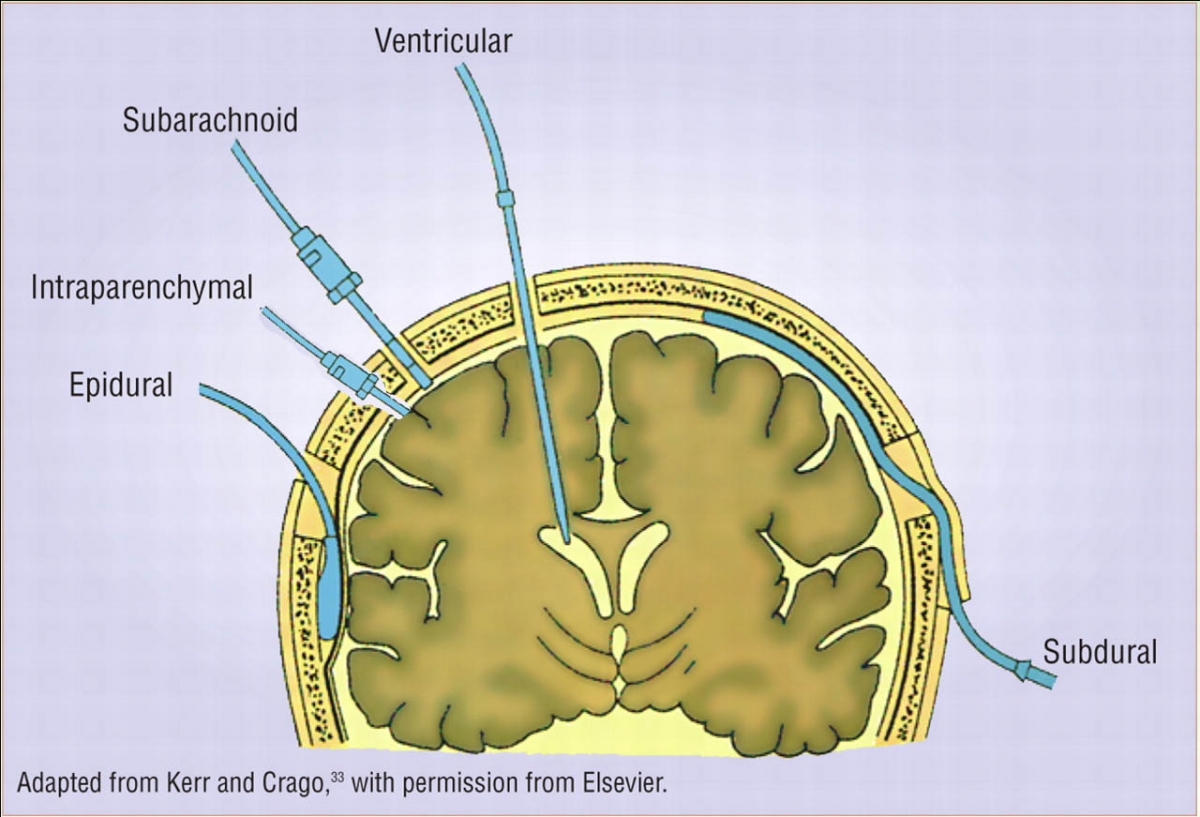
To measure the CPP you need and ICP (inter-cranial pressure monitor) which is a catheter through the skull into the brain and secured with a "bolt"
.
B/P requirement depend on each scenario. Head bleed being the more sensitive of the two as you need to maintain perfusion but control the B/P as an elevated B/P can cause more bleeding.
Don't go too far into that right now just be cognizant that it is a factor to keep in mins that you need a sufficient pressure to perfuse the brain but not so high that it can cause further damage.
Besides the patient identifiers and the order in the MAR, what do I need to check/assess/confirm before I hit this lady with a tPA bolus?[/QUOTE]
**Second independent check of order and dose calculations??
Funny, I actually wasn't thinking of that but yes, I did review the order and the dose with the pharmacist who was at bedside.
The two items of which I was specifically thinking were:
+ Signed consent form...
and
+ neuro check for baseline documentation prior to pushing the bolus.
The consent was signed...
but...
my neuro check found the sx to be nearly resolved...
I'm not pushing tPA on anybody whose symptoms have nearly resolved without the neurologist confirming the order... tPA is not to be trifled with...
I can't find the neurologist so I discuss with the pharmacist... who agrees with me that tPA-ing this lady is not the right decision at this point.
Finally, I find the neurologist and say, "this lady's symptoms have largely resolved." She replies, "Yeah, I'd expect them to." I say, "but we haven't given the drug yet..." She goes in, assesses the patient, and agrees that this patient no longer warrants tPA.
The patient was diagnosed with a TIA, scheduled for MRI/MRA, and admitted to a tele bed.
So, the lesson is: Reassess, reassess, reassess... and don't give a drug unless you're sure it's the right thing to do for that patient at that moment in time.
Interesting! So a TIA is not serious enough to warrant a dosage of tPA, correct? The patient would be given something else like an anticoagulant? I really need to review this stuff bc I'm already forgetting! :-/
Yes this was very interesting! These case scenarios also make me feel like I have learned zilch in nursing school (which is why I love these case scenarios, I learn a LOT from them).
So thanks again to you and Esme for taking the time to post on these! :)
This was very interesting. Didn't put my two cents in because.... Well I didn't have any. Waaaaayyyyy over my little paramedic head. Anway I would love to see more of these scenarios posted. Thanks for the post!!!!



 (which is why I love these case scenarios, I learn a LOT from them).
(which is why I love these case scenarios, I learn a LOT from them).
smf0903
845 Posts
Only thing I can think of is pregnancy, but I said that already so maybe given birth recently??