- Community
-
Programs
- Schools
-
Careers
- RN Specialties
- Best RN Jobs and Salaries
- Aesthetic Nurse
- Nursing Informatics
- Nurse Case Manager
- NICU Nurse
- Forensic Nurse
- Labor and Delivery Nurse
- Psychiatric Nurse
- Pediatric Nurse
- Travel Nurse
- Telemetry Nurse
- Dermatology Nurse
- Nurse Practitioner
- Best NP Jobs and Salaries
- Family NP (FNP)
- Pediatric NP
- Neonatal NP
- Oncology NP
- Acute Care NP
- Aesthetic NP
- Women's Health NP
- Adult-Gerontology NP
- Orthopedic NP
- Emergency NP
- Psychiatric-Mental Health NP (PMHNP)
- APRN
- Nurse Educator
- Nurse Administrator
- Certified Nurse Midwife (CNM)
- Clinical Nurse Specialist (CNS)
- Certified Registered Nurse Anesthetist (CRNA)
- Resources
- Education


melissamauzey
4 Posts
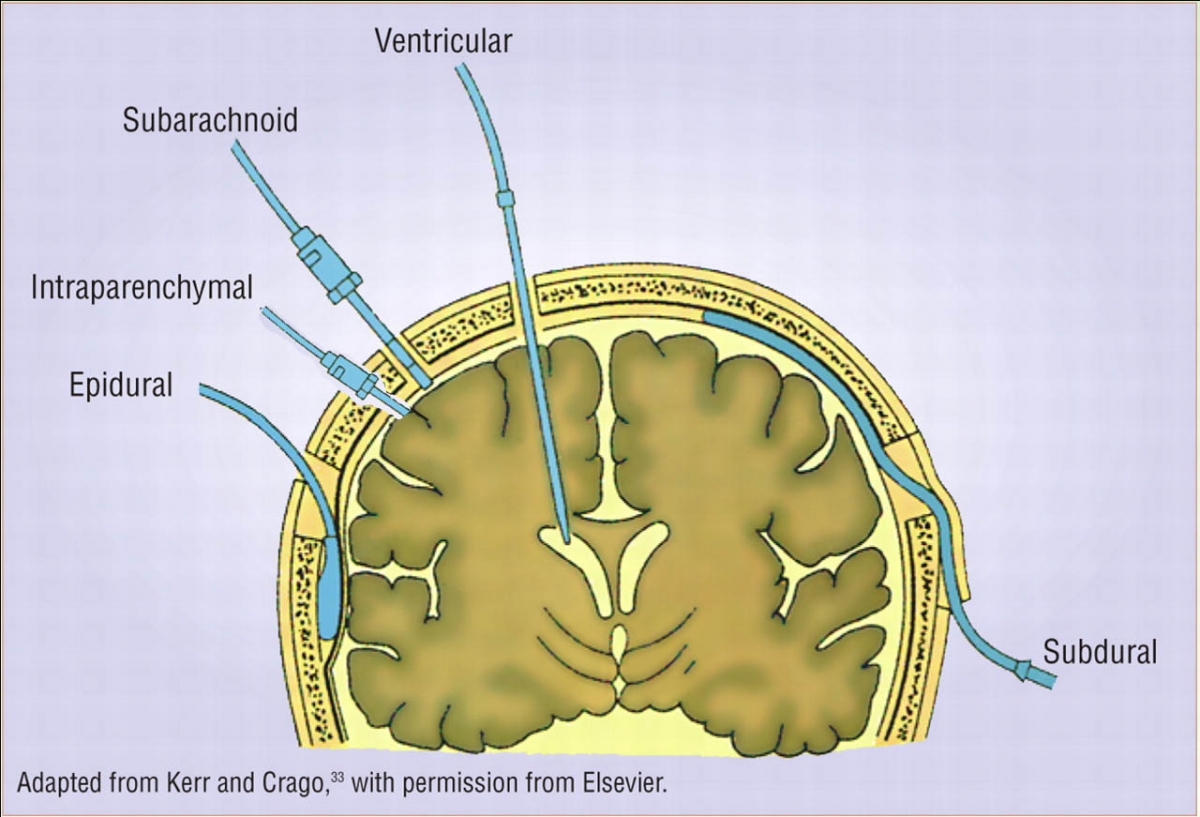
I chose the topic of external intracranial monitoring and drainage devices as a teaching topic for my PN teaching project. I'm way over my head. I've spent hours trying to understand the nurses responsibility and how and why she levels, zero's out, .....I'm in over my head. I need this in Dummies terms. I am writing a 5 page paper and am to give a 10 minute presentation....Please have mercy and help me...BTW...icufaqs.com: icp monitoring was over my head too.