- Community
-
Programs
- Schools
-
Careers
- RN Specialties
- Best RN Jobs and Salaries
- Aesthetic Nurse
- Nursing Informatics
- Nurse Case Manager
- NICU Nurse
- Forensic Nurse
- Labor and Delivery Nurse
- Psychiatric Nurse
- Pediatric Nurse
- Travel Nurse
- Telemetry Nurse
- Dermatology Nurse
- Nurse Practitioner
- Best NP Jobs and Salaries
- Family NP (FNP)
- Pediatric NP
- Neonatal NP
- Oncology NP
- Acute Care NP
- Aesthetic NP
- Women's Health NP
- Adult-Gerontology NP
- Orthopedic NP
- Emergency NP
- Psychiatric-Mental Health NP (PMHNP)
- APRN
- Nurse Educator
- Nurse Administrator
- Certified Nurse Midwife (CNM)
- Clinical Nurse Specialist (CNS)
- Certified Registered Nurse Anesthetist (CRNA)
- Resources
- Education

dano
76 Posts
I started working for a well known local hospital as a nurse extern I (some places call them nurse tech's, I've found it's not very uniform across the country). I've been in orientation for 2 weeks and worked 2 8-hour shifts so far. What a mad house, but I'm loving it! It feels great to have a job that actually matters (used to work retail) and the pay is none too shabby on top of it.
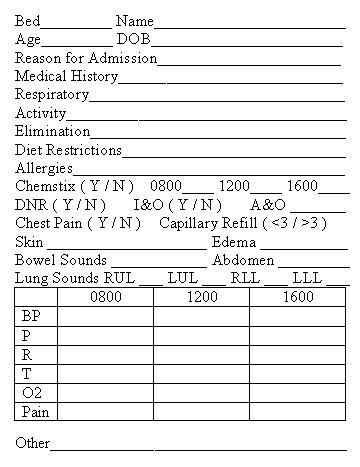
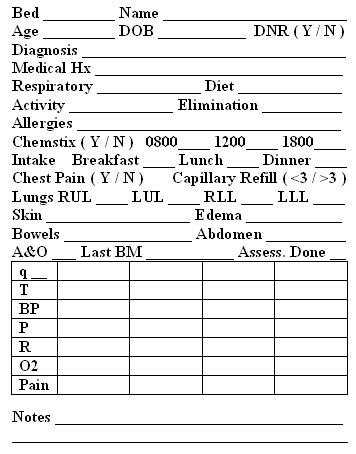
Anyways, I have noticed that most nurses run around with a blank piece of white paper and just scribble nonsense onto it (I'm sure it means something to them after years of experience). I used to find myself trying it during clinical and it was just a mess. I finally came up with a standard format I write out every morning, and after work today I turned it into a printable Word document.
Obviously it can also be modified for other times. I work either 7-3 or 7-7 so that's what works for me.
Has anyone else done this, care to post yours or tell me what you included?
I'm also curious if there's anything I'm leaving out that YOU would have to have on there in order to make use of it every day. I've sat in a few collaborative meetings and my RN preceptor's used my sheet instead of theirs because it was so detailed. I'd like to include as much as I can without making it super huge. Right now I can fit 4 of those on one 8x10 piece of paper with some space in the columns.
Thanks gang.