- Community
-
Programs
- Schools
-
Careers
- RN Specialties
- Best RN Jobs and Salaries
- Aesthetic Nurse
- Nursing Informatics
- Nurse Case Manager
- NICU Nurse
- Forensic Nurse
- Labor and Delivery Nurse
- Psychiatric Nurse
- Pediatric Nurse
- Travel Nurse
- Telemetry Nurse
- Dermatology Nurse
- Nurse Practitioner
- Best NP Jobs and Salaries
- Family NP (FNP)
- Pediatric NP
- Neonatal NP
- Oncology NP
- Acute Care NP
- Aesthetic NP
- Women's Health NP
- Adult-Gerontology NP
- Orthopedic NP
- Emergency NP
- Psychiatric-Mental Health NP (PMHNP)
- APRN
- Nurse Educator
- Nurse Administrator
- Certified Nurse Midwife (CNM)
- Clinical Nurse Specialist (CNS)
- Certified Registered Nurse Anesthetist (CRNA)
- Resources
- Education

Med-SurgRN311, BSN
2 Posts
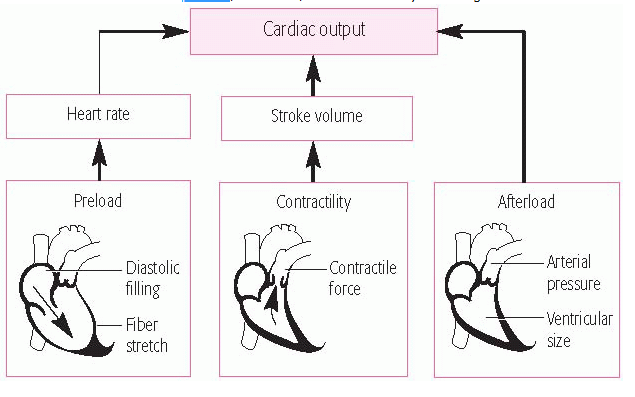
It would not be decreased afterload because that would indicate that it is easier for the heart to move blood out. Decreased afterload equals decreased resistance, meaning it is easier for the heart to pump blood to the systemic circulation. Any medication that causes vasodilation has this effect. An occluded coronary artery and the ischemia that results decreases contractility. Contractility and preload are related, the relationship described in Starling's Law. Increased preload leads to increased contractility to a point, after which contractility decreases, picture a balloon blown up several times until it loses its elasticity. Damage to the heart inherently reduces contractility, decreasing overall Cardiac Output. Blood and fluids backing up into the systemic/pulmonary circulation as in heart failure further increases preload and decreases contractility.