- Community
-
Programs
- Schools
-
Careers
- RN Specialties
- Best RN Jobs and Salaries
- Aesthetic Nurse
- Nursing Informatics
- Nurse Case Manager
- NICU Nurse
- Forensic Nurse
- Labor and Delivery Nurse
- Psychiatric Nurse
- Pediatric Nurse
- Travel Nurse
- Telemetry Nurse
- Dermatology Nurse
- Nurse Practitioner
- Best NP Jobs and Salaries
- Family NP (FNP)
- Pediatric NP
- Neonatal NP
- Oncology NP
- Acute Care NP
- Aesthetic NP
- Women's Health NP
- Adult-Gerontology NP
- Orthopedic NP
- Emergency NP
- Psychiatric-Mental Health NP (PMHNP)
- APRN
- Nurse Educator
- Nurse Administrator
- Certified Nurse Midwife (CNM)
- Clinical Nurse Specialist (CNS)
- Certified Registered Nurse Anesthetist (CRNA)
- Resources
- Education

Beau&B
5 Posts
Hi everyone!
I am a new grad starting next month on a cardiovascular surgical unit. I wanted to pick your brains!
*I currently have a littmann lightweight. Will this work for a cardiac floor, or should I buy a classic or a cardiology?
*What education/resource material should I buy? I am already looking through cardiovascular care made incredibly easy.
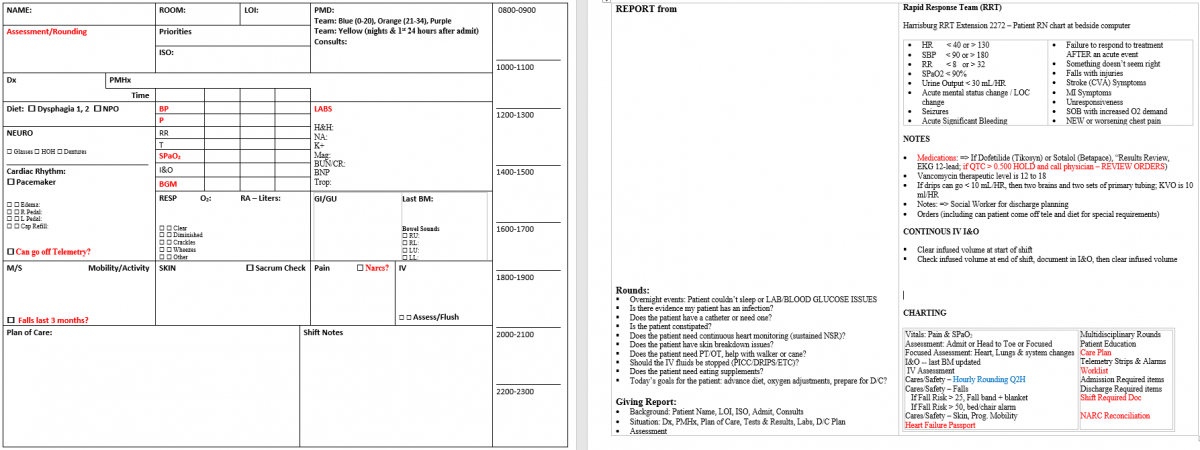
*Time management tips? Brain sheets?
*What NOT to do as a new grad in general?
My unit does 6 weeks of orientation on the floor, plus a basic dysrhythmia class. Thankfully I know some of the nurses there, so I feel like I will have a couple of support people.
Thank you!