- Community
-
Programs
- Schools
-
Careers
- RN Specialties
- Best RN Jobs and Salaries
- Aesthetic Nurse
- Nursing Informatics
- Nurse Case Manager
- NICU Nurse
- Forensic Nurse
- Labor and Delivery Nurse
- Psychiatric Nurse
- Pediatric Nurse
- Travel Nurse
- Telemetry Nurse
- Dermatology Nurse
- Nurse Practitioner
- Best NP Jobs and Salaries
- Family NP (FNP)
- Pediatric NP
- Neonatal NP
- Oncology NP
- Acute Care NP
- Aesthetic NP
- Women's Health NP
- Adult-Gerontology NP
- Orthopedic NP
- Emergency NP
- Psychiatric-Mental Health NP (PMHNP)
- APRN
- Nurse Educator
- Nurse Administrator
- Certified Nurse Midwife (CNM)
- Clinical Nurse Specialist (CNS)
- Certified Registered Nurse Anesthetist (CRNA)
- Resources
- Education




Factory Ten
3 Posts
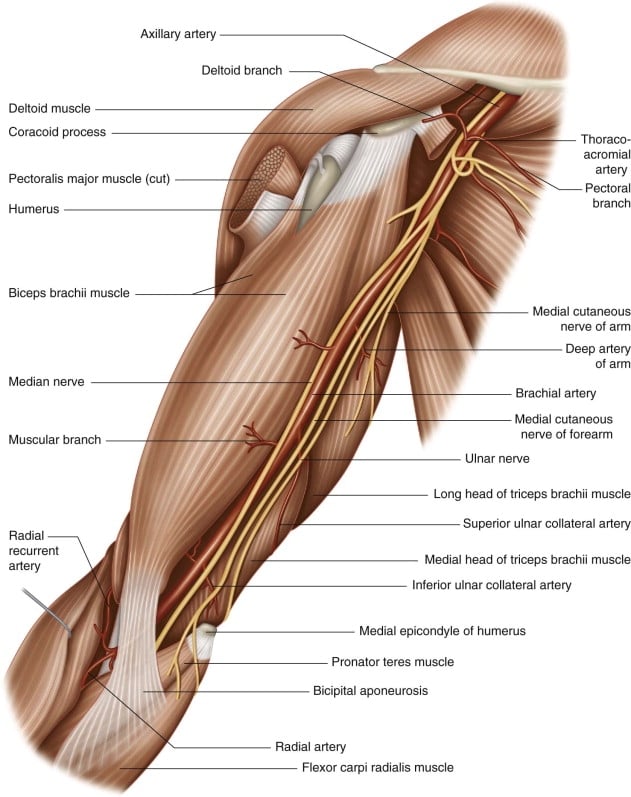
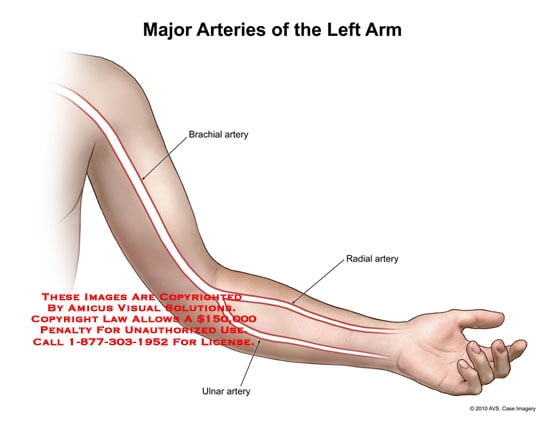
Today in class we began learning about taking vital signs. When it comes to pulses, though, I've been having a lot of trouble. I can only find the brachial and radial pulses occasionally. And when I try to hear the brachial pulse through my stethoscope, I simply can't. Its the latter issue that's really frustrating me.
Is it commonly possible to auscultate the brachial pulse without the BP cuff being attached and partially inflated? Or is this a sound that I'd most likely only hear with a higher-end stethoscope?