I am a 3rd semester RN 'A' level student. I have discovered that though I am good with theory learning and do well with NCLEX study questions, I am struggling with my clinical performance.
It seems that in carrying out patient care, I am "behind" schedule and need a better system of approach to my shift responsibilities. One barrier is that I am experiencing nerves and anxiety symptoms that I haven't had before because of the demeaning methods of my clinical instructor.
My heart starts pounding as soon as I see her. I want to learn, I'm eager to become a good nurse. I spend more hours in campus lab than anyone else to master skills. However, I believe my weakness is an organized execution of my duties.
We have been told that this is the semester is the semester to "show them what we got" meaning we should somehow have this organized approach to multi-tasking down already. Some of us do - like the ones who were CNA's for years.
That Isn't me.
And I don't seem to be learning how to develop this when I am barraged with criticism rather than offered support and true teaching. I wish there was a blue print or flow chart that teaches folks like me how to approach prioritization of care in an atmosphere of multiple priorities; I'm not getting it through mentorship - I just feel like I've been dumped on the floor and expected to perform beyond my current capabilities, under pressure, and without a road map.
I was told by my advisor that some students like myself just hit a wall in this semester and can't continue.
I've worked too hard!
I'm a good critical thinker!
Does anyone have any suggestions for remediation? Books, videos, etc. that address this and might help me help myself?
Thanks so much. I know I can do this with the right help !
We do work up to four patients by the end of the semester, not the beginning. First day or two, it is one patient. Second week, it is two and we stay there for a couple of weeks then it is three patients for several more weeks, then four towards the end. At the time I withdrew at 8 weeks, I was having trouble going from 2 to three patients - I was beginning to make mistakes and getting frazzled because I was starting to fear my instructor and my brain would just freeze. Interestingly, my peers in other clinical groups with other instructors were not hitting the wall I was hitting in this particular semester.
My first two semesters we worked from one the first semester to two the second semester. I didn't have this anxiety those first two semesters. My instructors were tough but I didn't fear them and they gave good and positive feedback in addition to criticism. They helped me believe in myself. So to answer your question about new floors - We get rotated on the different floors in an unpredictable manner at the beginning of the semester so by the end of my shift on one floor, I have gotten used to the layout but one week later, I would be on a different floor. Then might end up on that original floor the following week but I've lost some of my familiarity by then and there is some backtracking and retracing steps again. Many of us could be released to work with our primary nurses. My instructor kept a tight hold on me which I believe made matters worse as she wasn't bringing out the best in me - so was helping to create crisis. I really needed a breather from her so that my brain could function like I knew it could. But again, I don't do well if I am pushed more quickly than I am ready anyway so it made sense to try and redo this semester, recover from my downfall, and get a new instructor for the fall. I hope I will be in a better place to handle the demand...also other instructors may be more patient and allow for individual differences.
You rock black sunflower! I am going to save what you've written (I'm new to this and must figure out if I can copy and paste what you've written (do I have you're permission??) so that I can apply it to my typical shift (assignments are NEVER completed by 630 so I would have to adjust accordingly and most night nurses will only report once, not sooner and when they're good and ready -- when they're dealing with a student. Some are more cooperative). You've given me more guidance than I have gotten from my instructor...when we started the third semester, she said - "this is the semester that you need to 'show us what you got' " meaning we were expected to be able to know to do this as you've laid out. Ostensibly within a couple of weeks anyway.
I have done as you've recommended and then some with my instructor in terms of speaking to her in person, outside of clinical and after clinical to let her know how I best learn and that the pressure I was beginning to feel was starting to become the barrier, not the learning curve itself. I AM going to hang in there and hopefully my reputation with the rest of the instructors for next fall isn't too sullied that they will give me a fresh start to be successful. Thanks so much for your time to offer such a thorough plan!
When I was in clinicals 6 or 7 years ago, we were assigned our 1 or 2 patients the day before. We were allowed/encouraged to stop by the hospital unit the night before to look over their charts, med lists, care plans etc. That helped TREMENDOUSLY. I'd write down their diagnoses, meds & history and read up on everything, then arrive in the morning not totally clueless!
Is there any way to ask if this is possible?
Also, BE ASSERTIVE with your instructor. If the hospital policy is 1 hour before/after med admin, and she says otherwise, look her right in the eye, smile, and say, "hospital policy dictates that one hour before or after is acceptable." Some might tell you not to push the envelope. I say push it when you are definitely in the right. I did, and not only was I left alone, my instructors told me later they respected me for it.
Hopefully this thread is helpful for other instructors to read. It's certainly helpful for me to write about it. I'm grateful for the honest feedback I am getting.
Yes, the night before, we have one patient that we do our prep work and thorough research on as you've described and present a short written clinical worksheet that takes a few hours to prepare. The next morning, one and then two more patients are added on the fly during report.
Your point is well taken about standing up for myself. I did try that tactfully yet there were some instances that weren't worth standing up for myself - sometimes it is just better to accept the criticism whether or not it feels fair if you have an instructor that seems to be triggered by you.
The pinnacle of my demise in my third semester was when I was flushing a saline lock to prepare to switch it to a pump infusion. It leaked clear saline under the clear tagederm - I simply couldn't identify it like I would if it had a blockage or if it infiltrated. But it leaked under the arm and gravity caused it to drip under the elbow where I couldn't see it for what it was. I thought it was a good teaching and learning moment as it was a tricky thing to identify for a novice like me who has only read about such a complication rather than see it with my own eyes.
My instructor pulled me off patient care immediately and to my shock, told me she would need to send me home rather than let me finish my shift. This is when I did look my instructor directly in the eye and I firmly stated, "I don't want to go home, I want to learn - you are my teacher, please teach me. I've been improving, I know I can be successful - why aren't you invested in my success??"
It was a pretty intense exchange but it saved me from going home; instead, she pulled me off patient care and allowed me to shadow her as she supervised and helped other students (during which time, I saw that one of my peers was about to give a deltoid IM injection into the subcutaneous tissue under the arm - my instructor verbally guided her to the proper anatomy without ill repercussions). That's when I realized that my instructor had a negative personal bias towards me and that my semester was going to be futile - she did not treat the other student like me. I was written up and within two weeks of that I withdrew because her scrutiny became more relentless and it ultimately broke me. I believe I earned her respect...but it was more important for her to be "right". She happened to be adjunct faculty and maybe she was trying to prove herself to the nursing department. To be fair to her judgment, it is true that as I was "breaking", I began making mistakes when she came to supervise me (contaminating tubing and having to replace, contaminating my sterile gloves and having to replace, having a sealed baggie of labeled pt meds drop out of the pt binder I was carrying and get picked up by another nurse, it made me look like a total bobble head that had no business being in nursing, I just sunk). Instructor case was made and I withdrew rather than risk imminent failure. I was an A- student prior to this. I want to learn to be a good nurse. I'm willing to remediate, put in extra hours outside of clinical practicing skills, but it is so much better for handling pressure when you sense that an instructor really wants you to succeed and recognizes what you're doing well or acknowledges your continued improvement.
I am grateful for having a forum to help me make sense of my educational experience.
I'm pretty sure the point of nursing school is to learn and be corrected on the mistakes you make (although of course you try to make as few as possible). I have never had a clinical instructor demean me for making mistakes, just compassionately help me. I feel empathy for your situation and hope you never have to meet that instructor again. Your patient load is much higher as a student than mine is too. School is a time to learn not be overwhelmed by the care of many patients, that is not an atmosphere that is conducive to learning. A better way for the instructor to have helped you improve would have been to walk you through what to do in the patients room, then take you aside outside of the room and have you explain what you could have done better or how could have picked up on what was happening to the patient quicker, something along those lines. Good luck to you, I'm sure you'll make a great nurse as you seem very pro-active.
You rock black sunflower! I am going to save what you've written (I'm new to this and must figure out if I can copy and paste what you've written (do I have you're permission??) so that I can apply it to my typical shift (assignments are NEVER completed by 630 so I would have to adjust accordingly and most night nurses will only report once, not sooner and when they're good and ready -- when they're dealing with a student. Some are more cooperative). You've given me more guidance than I have gotten from my instructor...when we started the third semester, she said - "this is the semester that you need to 'show us what you got' " meaning we were expected to be able to know to do this as you've laid out. Ostensibly within a couple of weeks anyway.
I have done as you've recommended and then some with my instructor in terms of speaking to her in person, outside of clinical and after clinical to let her know how I best learn and that the pressure I was beginning to feel was starting to become the barrier, not the learning curve itself. I AM going to hang in there and hopefully my reputation with the rest of the instructors for next fall isn't too sullied that they will give me a fresh start to be successful. Thanks so much for your time to offer such a thorough plan!
Sorry it took me so long to get back to you, I could not find this post. Yes, please save anything that will help you. Do you have brain sheets that you use? I can post mine on here so you can use it if you want.
Specializes in Acute Care Cardiac, Education, Prof Practice.
blacksunflower said:
Sorry it took me so long to get back to you, I could not find this post. Yes, please save anything that will help you. Do you have brain sheets that you use? I can post mine on here so you can use it if you want.
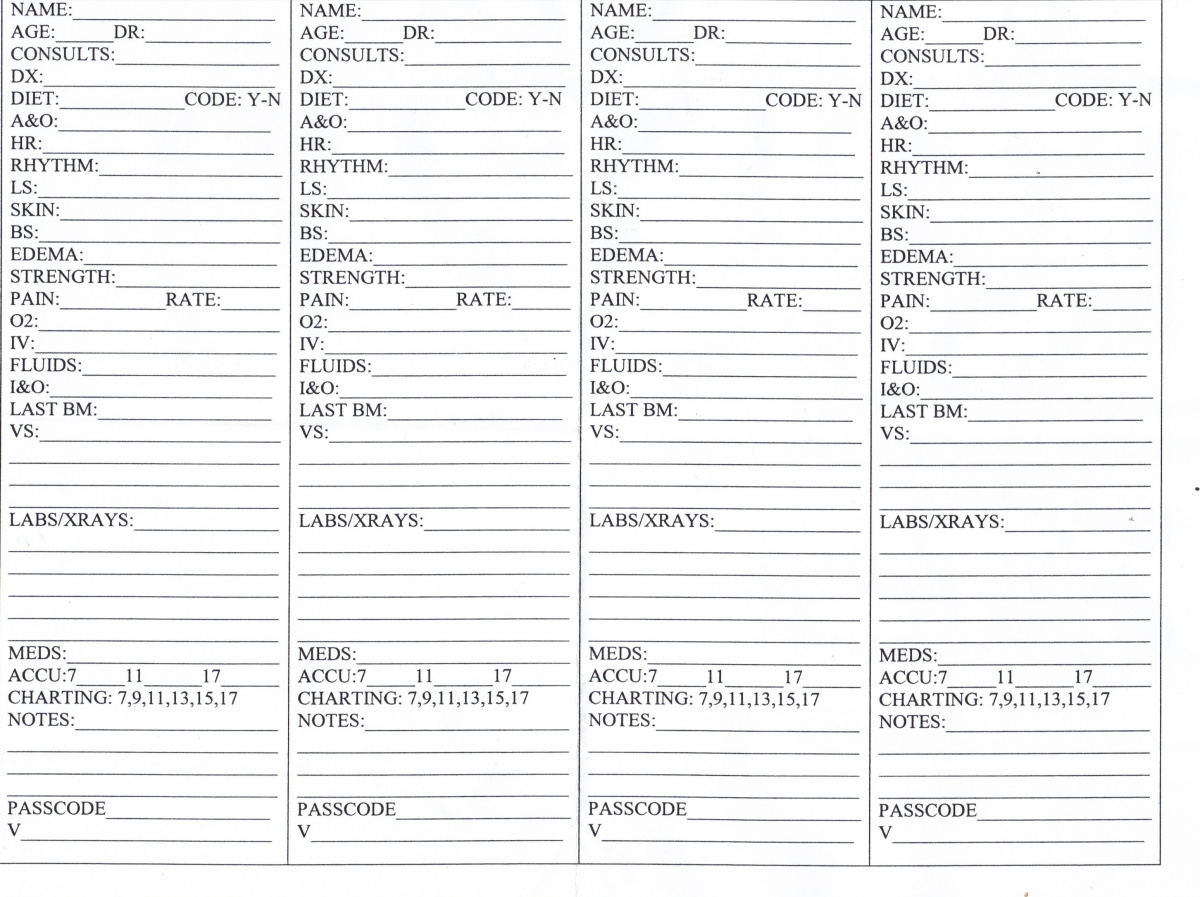
Good idea. Here is my sheet, though I swear it fits on one page when I print it off.
You have been very helpful. I have not quite landed on ideal brain sheets. I am definitely grateful to see what you are using. I'm not good at remembering the patient specifics without them - I'm stretched too thin for where I'm at in my development.
Sorry it took me so long to get back to you, I could not find this post. Yes, please save anything that will help you. Do you have brain sheets that you use? I can post mine on here so you can use it if you want.

onewill
21 Posts
We do work up to four patients by the end of the semester, not the beginning. First day or two, it is one patient. Second week, it is two and we stay there for a couple of weeks then it is three patients for several more weeks, then four towards the end. At the time I withdrew at 8 weeks, I was having trouble going from 2 to three patients - I was beginning to make mistakes and getting frazzled because I was starting to fear my instructor and my brain would just freeze. Interestingly, my peers in other clinical groups with other instructors were not hitting the wall I was hitting in this particular semester.
My first two semesters we worked from one the first semester to two the second semester. I didn't have this anxiety those first two semesters. My instructors were tough but I didn't fear them and they gave good and positive feedback in addition to criticism. They helped me believe in myself. So to answer your question about new floors - We get rotated on the different floors in an unpredictable manner at the beginning of the semester so by the end of my shift on one floor, I have gotten used to the layout but one week later, I would be on a different floor. Then might end up on that original floor the following week but I've lost some of my familiarity by then and there is some backtracking and retracing steps again. Many of us could be released to work with our primary nurses. My instructor kept a tight hold on me which I believe made matters worse as she wasn't bringing out the best in me - so was helping to create crisis. I really needed a breather from her so that my brain could function like I knew it could. But again, I don't do well if I am pushed more quickly than I am ready anyway so it made sense to try and redo this semester, recover from my downfall, and get a new instructor for the fall. I hope I will be in a better place to handle the demand...also other instructors may be more patient and allow for individual differences.