Adult Critical Care Update: New Definitions of Sepsis and Septic Shock
The proceeding article discusses new changes to the current definition of sepsis and septic shock and new tools for assessing patients are at risk from a recent publication by an international task force on sepsis.
If you haven't already read or heard about it, the Society of Critical Care Medicine and the European Society of Intensive Care Medicine have released a new document called Sepsis-3 otherwise known as the Third International Consensus Definitions for Sepsis and Septic Shock in late February 2016. As members of the healthcare team, we all strive to improve the prompt identification and treatment of sepsis as it continues to be a leading cause of mortality and ICU admission. Those on the financial end of healthcare are just as involved because sepsis accounts for a large cost of in-hospital care.
Because there is no single diagnostic test that identifies a patient as septic, previous definitions of sepsis relied heavily on the systemic inflammatory response that patients with sepsis exhibit. The Systemic Inflammatory Response (SIRS) Criteria were widely used as a screening tool to identify those patients who may have sepsis. Under the definitions we have been using, patients who meet 2 or more findings in the SIRS Criteria were further stratified into a tiered classification system based on severity that starts with (1) Sepsis, if they also have a suspected source of infection, (2) Severe Sepsis, if they met the criteria for Sepsis and have either signs of end organ damage, hypotension (SBP Levy et al, 2003)
Many of us in Critical Care and those who work in Rapid Response Teams are familiar with this language. I'm very certain that nurses have filled out countless sepsis screening forms and triggered hospital-wide sepsis activation pages using these tools.
Recent research, have revealed that the criteria we've been using lacks the validity in predicting in-hospital mortality for sepsis (Seymour et al, 2016). I think those of us in clinical practice realize this even before the research findings were released. How many times have you triggered a sepsis alert on a patient meeting the SIRS Criteria, ongoing infection, and elevated lactate yet had other reasonable etiologies for such findings that do not necessarily go along with sepsis?
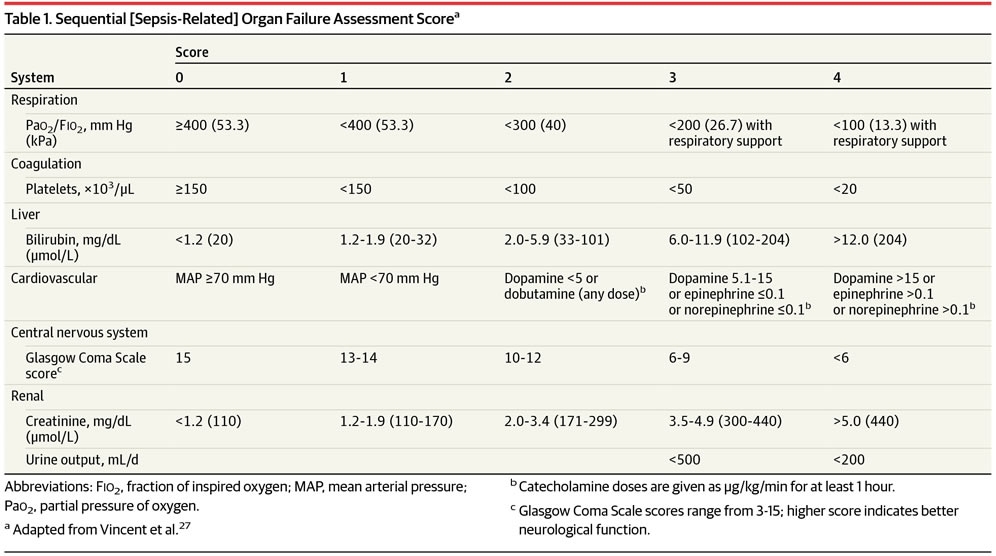
Sepsis-3 now defines sepsis as a "life-threatening organ dysfunction caused by a dysregulated host response to infection" (Singer et al, 2016)). A new tool to quantify organ dysfunction being proposed is the Sequential Organ Failure Assessment (SOFA).
Organ dysfunction is deemed present if there is an acute change in the total SOFA score ≥2 points consequent to the infection with the understanding that baseline SOFA score is zero in patients without known preexisting organ dysfunction. A quick SOFA (qSOFA) can be used as a quick tool for identifying those with a risk of mortality or requiring an ICU admission since SOFA relies on parameters not immediately available in some situations (i.e., non ICU patients). See below:
Finally, septic shock is now defined as a "subset of sepsis in which underlying circulatory and cellular/metabolic abnormalities are profound enough to substantially increase mortality. Patients with septic shock can be identified with a clinical construct of sepsis with persisting hypotension requiring vasopressors to maintain MAP ≥65 mm Hg and having a serum lactate level >2 mmol/L (18 mg/dL) despite adequate volume resuscitation" (Singer et al, 2016)).
With these new definitions and tools, we are likely to see an overhaul of our previous system of sepsis monitoring in our respective healthcare institutions. It may mean new forms that reflect these new definitions to fill out for sepsis screening. Feel free to express your thoughts.
Specializes in ACNP-BC, Adult Critical Care, Cardiology.
So is anyone trying to incorporate the new recommendations and definitions into their current sepsis protocols? If so, how are you reconciling the CME core measure reporting requirements that are based on the outdated info?
That's great question. I hope others can share what their individual facilities are doing. As it is, most EMR systems (such as Epic) still trigger sepsis alerts based on SIRS criteria. I have not been "in the know" regarding the transition in terms of EMR systems but I'm sure there are requests by clinicians to upgrade based on these new recommendations. I would say though that existing quality measures (such as cultures drawn and antibiotics started within the hour of identification) will remain the same.
You have to really watch for patients like me :-/ Because I'm a nurse, and hard headed, I almost died from septic shock, because I walked around for days being "ok." I had my appendix out and started feeling crummy again a few days later. Had seen the surgeon post-op days 2 and 9. On the 10th day I drug myself out of bed, drove an hour and a half to a teaching facility for a FHM class that I needed. I didn't make it all the way through the class. They hauled me down the hall to the ER where I was on my way to meet my maker! The doctor referred to me as an exotic bird. No matter how sick they get, they will fight to stay alert and "healthy" so they don't get eaten by predators. (Survival instincts.) (Or stubborn nurse syndrome.) What brought me around coherent enough to talk to my caregivers, was the excruciating pain the blood pressure cuff caused! It felt like every bone in my entire arm was being crushed.
Everyone's coming in with "sepsis" these days . Pt tachy 114, SBP 88 sepsis. Early recognition most definitely saves lives, but often times formulas and protocols remove common sense and actually looking at the patient at bedside. I wise healthcare provider knows when to use formulas / protocols and when not to. Recently heard a study quoted that looked at ACS EBP. They looked at the definitive study for things live heparin or aspirin admin in ACS and the average length of time is took from the publication of the study to implementation by 75 and 90 % of hospitals and for guidelines to be published. This is staggering but it took and average of 16 years from the time of the definitive publication to implementation. That gap is too big and I'm afraid many of our protocols fall into things like that "well this is the protocol, this is how we do it here". BUT WHY?

Corey Narry, MSN, RN, NP
8 Articles; 4,491 Posts
That's great question. I hope others can share what their individual facilities are doing. As it is, most EMR systems (such as Epic) still trigger sepsis alerts based on SIRS criteria. I have not been "in the know" regarding the transition in terms of EMR systems but I'm sure there are requests by clinicians to upgrade based on these new recommendations. I would say though that existing quality measures (such as cultures drawn and antibiotics started within the hour of identification) will remain the same.