Short Circuit: Supraventricular Tachycardia for the Novice PICU Nurse
This article is intended to provide a basic understanding of supraventricular tachycardia (SVT) and its treatment. Pediatric patients are managed a little differently from big people. The article covers adaptations to the developmental stages of children in treating this pediatric emergency.
Let's pretend you're working on a pediatric inpatient unit and one of your patients was admitted for the ubiquitous and poorly-defined failure-to-thrive syndrome. This little kiddo is 5 months old and weighs 4 kg, so obviously not a robust and chubby individual. Physical exam of Julie, as we'll call our hypothetical patient, is essentially normal except for her small stature. She seems to have a good appetite but rarely finishes a bottle. While feeding she sometimes becomes pale and tachypneic, and generally looks unwell. But so far nothing has been definitively identified as a cause of this phenomenon.
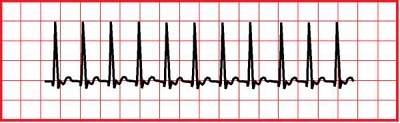
You're making your rounds in the early afternoon when Julie's mom rushes up to you in a bit of a panic, Julie lying pale and limp in her arms. Your first action is to call for the rapid response team and take Julie to the treatment room. You strip off her sleeper and see that she's mottled and her extremities are cool to the touch. She is breathing, at a rate of 40 and with moderately increased effort. Her eyes are closed and she isn't responding much to the activity around her. You check for a brachial pulse and feel one but can't count it. You put her on the treatment room monitor and this is what you see:
The monitor ECG gives you a rate of 246; BP is 62/48, RR still 40 and her O2 sat is 91%. What do you do next?
Julie is in supraventricular tachycardia (SVT). The first clue comes from all those signs of poor perfusion. The ECG tracing shows a very fast, regular rhythm with no visible P waves that can't be explained by pain or agitation, since Julie is limp and almost unresponsive. The usual adult treatment - asking the patient to bear down - isn't going to work for Julie because she's way too young to understand your directions. But she's a baby; babies and small children retain the primitive mammalian dive reflex, so you can take advantage of that. You shout out to one of your coworkers to bring you some ice, and while you're waiting, you put Julie supine on the treatment room exam stretcher. You quickly bring her knees tightly up to her chest and press her legs gently but firmly up against her abdomen. Watching the monitor you see no change so you try it again. The ice arrives and you ask your coworker to apply the bag of ice directly to Julie's face. The shock of the cold bag against her skin momentarily interrupts her fast rhythm and for about a minute she has a normal sinus rhythm at a rate of 140. That's still a little fast but well within the expected range for her age. You start to relax, but just as the RRT arrives on the scene, Julie's heart rate spikes again to 250. Rats!
The RRT takes over. The respiratory technologist applies oxygen to Julie's face via blow-by and the nurse does a quick assessment. She's already done a primary survey of the situation as she came through the door so she knows about the SVT. She tells you that you've done everything correctly to this point but Julie is going to need advanced intervention. She pops in an IV and administers adenosine via direct IV push. For what seems like an eternity, Julie's ECG is a flat line. Then her heart starts beating again at a rate of 134. The RRT prepare her for transfer to the PICU and thank you for your help.
Supraventricular tachycardia is an abnormally conducted rhythm originating in the atrio-ventricular node, rather than in the sinus node. Since the electrical impulse has a much shorter distance to travel by this pathway, the rate speeds up. The faster the heart beats, the less able the ventricles are to fill with blood. The less blood the heart is able to circulate, the worse the patient looks. Blood pressure falls, level of consciousness follows and the patient needs rapid intervention.
Distinguishing SVT from the more run-of-the-mill sinus tachycardia isn't difficult if the patient is being monitored. First of all, changes in rate are sudden and are independent from the patient's state. That means the rate increases instantly without obvious cause. The child may even be asleep when it occurs. Secondly, this rapid rate is perfectly regular. And it exceeds the threshold for sinus tachycardia, which is 230 beats per minute for infants and 180 beats per minute for older children.
Emergency treatment utilizes vagal manoeuvres which can be achieved by bearing down as though to have a bowel movement, by pretending your thumb is a balloon and trying to blow it up or the knee-to-chest manoeuvre described above. Eliciting the dive reflex also produces a vagal response and may slow the heart rate. If these measures fail, a rapid intravenous bolus dose of adenosine may arrest the abnormal rhythm. Initial dose is 0.1 mg/kg to a maximum of 6 mg; if that dose fails, a second dose of 0.2 mg/kg to a maximum of 12 mg may be given. If adenosine fails, the next step may be to administer an antiarrhythmic drug such as amiodarone. This would be the treatment of choice for a patient with refractory SVT who has relatively adequate perfusion because of the time required. The dose is 5 mg/kg infused over 20-60 minutes.
The physician may choose to move to synchronized cardioversion if the patient's overall condition won't allow the delay needed for amiodarone. If If electrical cardioversion is required and time allows, give the patient some sedation because it's going to hurt! The initial dose is 0.5-1 joules/kg. Bedside monitoring must be continued during cardioversion as the defibrillator's Quik-Combo pads can only accomplish one task at a time. They're either monitoring a rhythm or they're delivering a shock. It's also important to ensure the defibrillator has the power dial set to "SYNC" to allow the shock to be delivered at the right point in the cardiac cycle. Shocking at the wrong time could result in the dreaded R-on-T phenomenon where the shock is delivered before the ventricles have repolarised - and you'll really be in the soup then... the heart won't have a clue what to do next. Follow all the steps in the right sequence and your patient will be safe. Now, if the first shock wasn't effective to convert the rhythm, double the dose of electricity to 1-2 joules/kg and shock again.
Most kids will convert with one or more of the described measures. But some of them will continue to be refractory. These children may then be given a continuous infusion of amiodarone at a dose of 2.5-5 mcg/kg/min, gradually increased to as high as 20 mcg/kg/min as required. Amiodarone has a very long half life so weaning isn't absolutely necessary. If amiodarone fails the child will have an electrophysiological study to determine the exact location of the aberrant pacemaker, then a trip to the cath lab for ablation of that patch of tissue.
In an emergency a good rule of thumb is to check your own pulse first. It's difficult to perform skillfully and efficiently when you're having a meltdown. Keep your head about you and both you and your patient will survive!
Thank you for writing this article! It was very informative, and easy to undertand. Although I am not a pediatric nurse, its always nice to learn new things!
One of the scariest NICU transfers I was ever a part of was an 18hr old newborn in SVT. Two doses of adenosine later he was back in NSR and obviously cards followed him after d/c.
elixRN, BSN, RN
1 Article; 23 Posts
Thank you for writing this article! It was very informative, and easy to undertand. Although I am not a pediatric nurse, its always nice to learn new things!